





Abstract
Follicular pancreatitis (FP) is characterized by nodular mass composed of lymphoid hyperplasia and fibrosis. We here present radiological and pathological features of three cases of FP. The three patients were middle- or old-aged men, and nodular mass was pointed out at health examination. Computed tomography failed to demonstrate a mass. Magnetic resonance imaging demonstrated a mass in each case. 18F-fluorodeoxyglucose positron-emission tomography (FDG-PET) demonstrated two nodular masses with high standardized uptake value (SUV) in two cases and single mass in one case. The pathological examination disclosed two lesions with fibrosis and hyperplastic lymphoid follicles in two cases and one lesion in one case. Masses with high SUV appeared to correspond with the lesions of FP. Compared with the features of FDG-PET images of pancreatic ductal carcinoma, multiple lesions with high SUV favor a diagnosis of FP rather than pancreatic cancer. FDG-PET is useful for the diagnosis of FP.
INTRODUCTION
Follicular pancreatitis (FP) is a rare disease, and only 15 cases were reported in the literature [1–7]. FP forms a nodular mass in the pancreas, and the lesion is characterized by fibrosis and lymphoid hyperplasia with prominent germinal center [1]. In most of cases, the masses were incidentally found by health examination. It is difficult to differentiate FP from pancreatic ductal carcinoma (PDC), and the patients underwent surgical resection of the pancreas. Because of the rarity of the disease, the radiological features of FP are not well known. The elucidation of features is helpful for the diagnosis of FP and may enable to avoid unnecessary surgical treatment. We here report radiological features of three cases of FP.
CASE REPORT
The three patients were middle- and old-aged men (Table 1). All patients had no symptoms, and a mass lesion was pointed out by abdominal ultrasound sonography (USG) at annual medical examination (Fig. 1A). Two patients received medication for hypertension and dyslipidemia (Cases 1 and 3). Two patients were smoker (Cases 2 and 3). Tumor markers (CEA, CA19-9, SPan-1 and DUPAN-2) were within normal limits in all cases.
Clinical and radiologic features
| Case# | Age/sex | # of lesion | Location | Size | CT | MRI | PET (SUV max) |
|---|---|---|---|---|---|---|---|
| 1 | 67/M | 2 | Body | 1.8 cm | ND | Low-intensity mass | 3.14 |
| Tail | 1.5 cm | ND | ND | 2.18 | |||
| 2 | 55/M | 2 | Body | 2.0 cm | ND | ND | 2.25 |
| Tail | 2.5 cm | ND | Low-intensity mass | 3.57 | |||
| 3 | 84/M | 1 | Body | 2.3 cm | ND | Low-intensity mass | 3.19 |
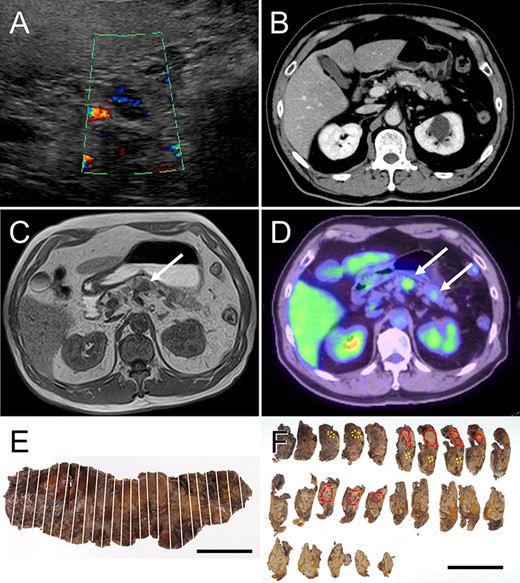
Radiological features and macroscopic findings of Case 1. (A) Abdominal ultrasonography: hypoechoic mass was demonstrated in the pancreas. (B) CT: no mass lesion was detected. (C) MRI: T1-weighted image showed nodular mass of low intensity (white arrow). (D) FDG-PET: two nodular masses with high SUV were detected in the pancreas (white arrows). (E) The macroscopic appearance of the resected pancreas. (F) Two nodular lesions (red circles) and foci of small lesions (yellow circles) were determined by histological examination on the cut surface.
A nodular mass was noted in the body or tail of the pancreas by USG in three cases (Figs 1–3). Endoscopic ultrasound-guided fine needle aspiration gave negative result in all patients. No lesion was detected by computed tomography (CT) (Fig. 1B and Table 1). Low-intensity mass was detected in the body or tail with T1-weighted imaging of magnetic resonance imaging (MRI: Fig. 1C and Table 1). 18F-fluorodeoxyglucose positron-emission tomography (FDG-PET) detected two lesions with high standardized uptake value (SUV) in the body and tail in Cases 1 and 2 (Figs 1D and2A and Table 1) and one lesion in the body in Case 3 (Fig. 3A and Table 1). In the resected pancreas, two lesions were found in the body and tail of the pancreas in Cases 1 and 2 (Figs 1F and2C, red circles) and one lesion of the pancreatic body in Case 3 (Fig. 3C, red circles). Small foci of lymphoid hyperplasia were noted in all cases (Figs 1F, 2C and3C, yellow circles).
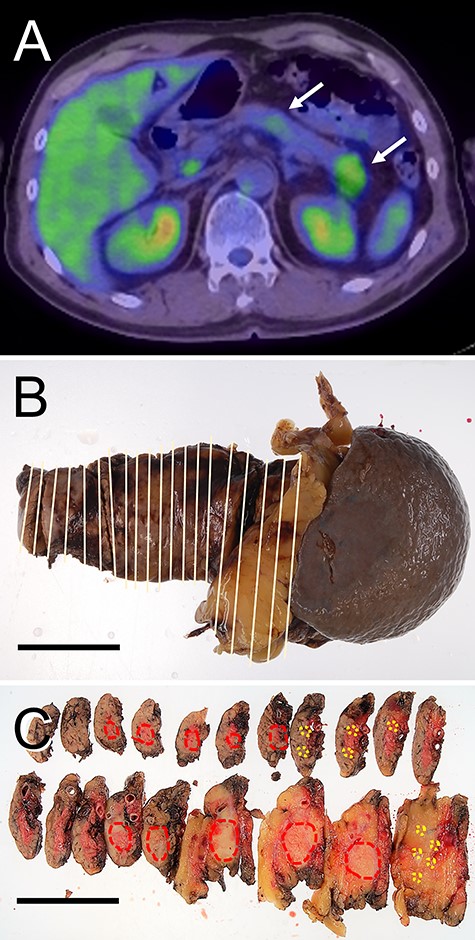
Radiological features and macroscopic findings of Case 2. (A) FDG-PET: two nodular masses with high SUV were detected in the pancreas (white arrows). (B) Macroscopic finding of the resected pancreas. (C) Two nodular lesions (red circles) and foci of small lesions (yellow circles) were indicated on the cut surface.
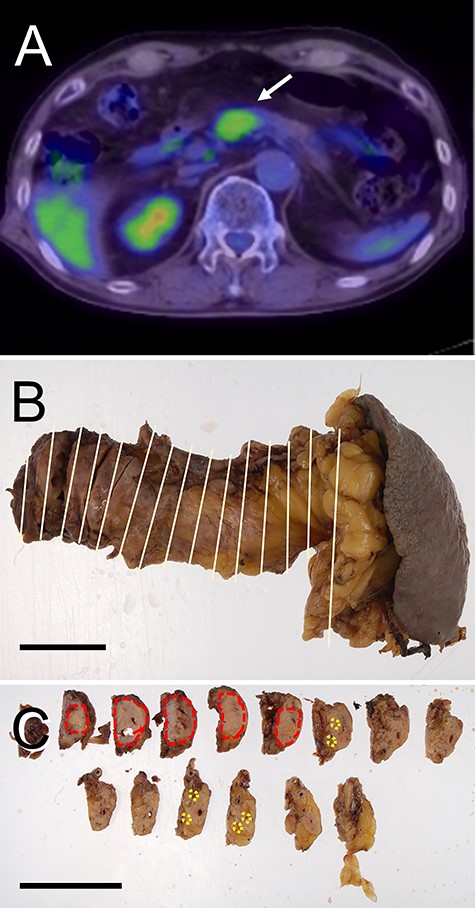
Radiological features and macroscopic findings of Case 3. (A) FDG-PET. (B) Macroscopic finding of the pancreas. (C) A nodular lesion (red circles) and foci small lesions (yellow circles) were indicated on the cut surface.
The location and SUV in 17 cases of PDC were reviewed and compared with those in the present cases (Table 2). The main lesions were multiple in two out of three cases of FP, whereas the lesion was single in PDC. The level of SUV was ~2.1 times higher in PDC compared with those in FP.
FDG-PET of FP and PDC
| Location | SUV max (mean ± SD) | Multiple lesions | |
|---|---|---|---|
| FP (n = 3) | B + T: two cases | 2.87 ± 0.55 | Two cases |
| B: one case | |||
| PDC (n = 17) | B:T = 12:5 | 5.89 ± 5.56 | Zero case |
B, body; SD, standard deviation; T, tail.
Representative histological features of the resected pancreas are shown in Fig. 4. The lesion was well demarcated fibrous tissue accompanied by numerous lymphoid follicles (Fig. 4A). The lymph follicles were associated with prominent germinal centers (Fig. 4B). The germinal center cells were negative for Bcl-2 (Fig. 4C). In addition, there are numerous tingible body macrophages. Numerous IgG-positive plasma cells were present in the lymphoid follicles (Fig. 4D), but only a few IgG4-positive plasma cells were present (Fig. 4D). These evidences suggested that the lymph follicles were reactive, and follicular lymphoma and IgG4-related disease were excluded. A diagnosis of FP was made in three cases.
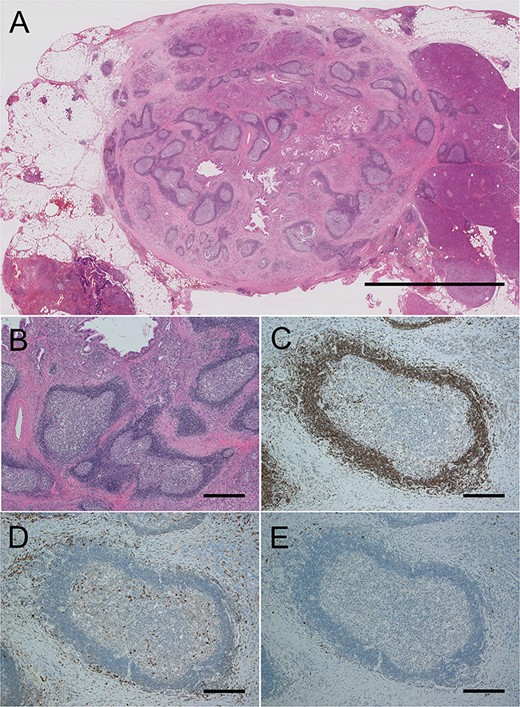
Histological findings of the pancreas in Case 1. (A) Loupe image of the large lesion of the tail. Scale bar, 1 cm. (B) High magnification of the lesion. Magnification, ×20; scale bar, 500 μm. (C) Immunostaining of Bcl-2 was negative in irregular germinal centers. (D) Many IgG-positive plasma cells could be seen. (E) IgG4-positive plasma cells were rarely seen. (D and E, ×100 magnification; scale bars 100 μm).
DISCUSSION
The present study demonstrated the radiological and pathological features of three cases of FP. The pathology of FP is characterized by multiple lesions, which were fibrous mass with reactive lymph follicles and varied in sizes. It should be noted that there are small lesions of the size < 1 cm in the resected pancreas. Multiple lesions were reported in four cases of FP [2–4, 7].
In our series of cases of FP, the lesions were not detected by CT, whereas the lesions were detected as low-intensity mass by MRI. This was paralleled with the previous reports that showed the usefulness of USG or MRI for the detection of the lesions [2–4]. In the current case study, it appeared that FDG-PET is useful for the detection of the lesions of FP. The detected mass corresponded the nodular lesion of FP in the resected pancreas. Two lesions were detected in Cases 1 and 2, and one lesion was detected in Case 3 by FDG-PET. It was not feasible to detect the lesions of the size smaller than 1 cm by FDG-PET.
To validate the usefulness of FDG-PET for the diagnosis of FP, the radiological features of FP by FDG-PET were compared with those of PDC (Table 2). Since lesions of FP were noted in the body and tail of the pancreas in the present study, the radiological features of PDC in the body and tail were reviewed. The SUV max of FP was high, but the SUV max of PDC was ~2.1 times higher than that of FP. Multiple lesions were detected in two of three cases of FP, whereas high-SUV lesion was solitary in all cases of PDC. When high-SUV lesion is detected in the body and/or tail of the pancreas and lesions are multiple, FP should be counted into consideration for the differential diagnosis. FDG-PET is useful for the diagnosis of FP.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
COMPLIANCE WITH ETHICAL STANDARDS AUTHORSHIP DECLARATION
This manuscript is not a duplicate publication and has been seen and approved by all authors.
INFORMED CONSENT
Informed consent was obtained from all individual patients.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
ETHICAL APPROVAL
This study followed the ethical guidelines of the Declaration of Helsinki. The study was approved by Ethical Committee of Nippon Medical School Hospital (B-2019-009).

{kind=link}
{kind=link}
{kind=link}
{kind=link}