





Abstract
An 81-year-old woman had undergone laparoscopic abdominoperineal resection for rectal cancer. A permanent colostomy was created through an intraperitoneal route. Three months after the surgery, the patient presented with lower abdominal pain and vomiting. Computed tomography showed gastric incarceration through the lateral space of the lifted sigmoid colostomy. Although the herniated stomach was reduced by nasogastric tube decompression, the patient experienced a recurrence of gastric hernia shortly thereafter. A laparoscopic operation was performed, and a new colostomy was constructed through an extraperitoneal route. The patient had no hernia recurrence during the 20 months of follow-up after the operation. Gastric internal hernia associated with colostomy can occur as a rare complication. Although reduction of the incarcerated stomach is possible by nasogastric tube decompression, surgical repair of the hernia may be the optimal management to prevent recurrence.
INTRODUCTION
Internal hernia is a rare condition defined by the protrusion of a viscus through an intraperitoneal aperture. The aperture can be formed congenitally or acquired postoperatively, as represented by Petersen’s hernia [1].
In abdominoperineal resection (APR) or Hartmann’s procedure for lower rectal cancer, a sigmoid colostomy is created most commonly through an intraperitoneal route. The lifted colostomy creates a new intraperitoneal space in the lateral side, and this space potentially causes an internal hernia. To date, there have been a few reports on internal hernia in the lateral defect of the colostomy [2–4]; all of the previously described cases of internal hernia associated with colostomy have shown a hernia of the small intestine. We herein describe the first case of gastric internal hernia through the lateral space of the colostomy after laparoscopic APR.
CASE REPORT
An 81-year-old Japanese woman had undergone laparoscopic abdominoperineal resection for rectal cancer. A permanent colostomy was created through an intraperitoneal route. Pathologically, the tumor was classified as pT2N0M0 [5], and R0 resection was achieved.
Three months after the surgery, the patient presented with lower abdominal pain and vomiting. Contrast-enhanced computed tomography (CT) showed gastric incarceration through the space between the lifted sigmoid colostomy and the left lateral abdominal wall (Fig. 1a). Because the incarcerated stomach had no evidence of strangulation, conservative therapy with nasogastric tube decompression of the dilated stomach was administered. A CT on the next day showed the reduction of the stomach (Fig. 1b), and oral intake was started. However, the patient again began vomiting on the 7th and 13th days after admission, and a CT on the 13th day revealed recurrence of the gastric hernia.
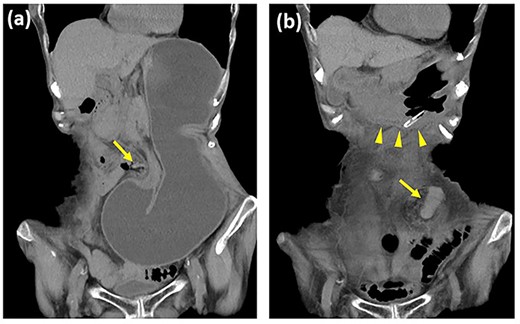
Contrast-enhanced computed tomography images of the gastric internal hernia. (a) The stomach is incarcerated through the lateral defect of the lifted sigmoid colostomy (arrow). (b) The stomach (arrowhead) is reduced after nasogastric tube decompression.
A laparoscopic operation was performed for the recurrent hernia. Intraoperative findings showed that the gastric hernia had been reduced and ischemic changes were not evident in the stomach (Fig. 2a). Because the lateral defect of the lifted sigmoid colostomy was too large for suturing closure, a new colostomy was constructed laparoscopically through an extraperitoneal route (Fig. 2b). The patient’s postoperative course was uncomplicated, and she had no recurrence of hernia within the 20 months of follow-up after the surgery.
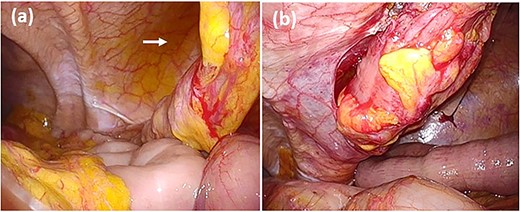
Intraoperative findings of hernia repair. (a) The gastric incarceration is not evident in the lateral space of the sigmoid colostomy (arrow) at the time of exploration. (b) The colostomy is reestablished through an extraperitoneal route using the same stoma site.
DISCUSSION
Colostomy formation is a common procedure still associated with a wide variety of complications. While parastomal hernia is one of the major stoma-related complications with an incidence ranging from 4–48% after end-colostomy formation [6], internal hernia associated with colostomy rarely occurs. The present patient is the first case of gastric internal hernia associated with colostomy. The key finding of this case was that revision of the colostomy was ultimately needed in the course of hernia recurrence.
There have been six case reports on internal hernia associated with colostomy, and all but the present patient showed hernia of the small intestine (Table 1) [2–4]. Although these reported herniated small intestine cases were all strangulated, immediate reduction by emergency surgery allowed for preservation of the strangulated small intestines with no mortality. Of note, two patients developed internal hernia even after colostomy creation through an extraperitoneal route [2, 3], which theoretically minimizes the risk of internal hernia by removing the defect between the lifted colon and the lateral abdominal wall. Therefore, internal hernia-associated colostomy is unlikely to be completely prevented, and selecting an optimal treatment is crucial when it occurs.
Reported cases of internal hernia through the lateral space of the lifted sigmoid colostomy
| Reference | Age (years), sex | Primary surgery, stomal route | Interval* | Herniated organ, condition | Treatment for hernia | Follow-up |
|---|---|---|---|---|---|---|
| Yokota et al. [2] | 70, M | Laparoscopic APR, extraperitoneal | 3 months | Small intestine, strangulated | Stoma revision with extraperitoneal route | Not available |
| Yokoyama et al. [3] | 56, M | Open APR, extraperitoneal | 9 days | Small intestine, strangulated | Direct suture repair | 21 months, no recurrence |
| Yasukawa et al. [4] | 70, M | Laparoscopic APR, intraperitoneal | 2 months | Small intestine, strangulated | Omental patch closure | Not available |
| Yasukawa et al. [4] | 75, M | Laparoscopic APR, intraperitoneal | 2 months | Small intestine, strangulated | No repair with reduction of the herniated intestine | 1 month, recurrence of hernia |
| Yasukawa et al. [4] | 83, M | Laparoscopic Hartmann’s operation, intraperitoneal | 15 months | Small intestine, strangulated | Stoma revision with intraperitoneal route | Not available |
| Present case | 81, W | Laparoscopic APR, intraperitoneal | 3 months | Stomach, not strangulated | Stoma revision with extraperitoneal route | 20 months, no recurrence |
M, man; W, woman; APR, abdominoperineal resection.
*Between primary surgery and hernia development.
In the present patient, the incarcerated stomach was smoothly reduced by nasogastric tube decompression, resulting in avoidance of emergency surgery. The successful reduction may be attributed to the large hernia defect and easy access to the herniated stomach by nasogastric tube. Unfortunately, the present patient showed early recurrence within 2 weeks, leading to a need for the patient to undergo a definitive surgical treatment. Although additional evidence is lacking, this result suggested that surgical repair of hernias should be selected at the time of the first gastric incarceration. If nonoperative management is chosen, careful observation for hernia recurrence is mandatory.
Surgical options for hernia repair include direct suture of the hernia defect [3], omental patch [4] or revision of the colostomy through an extraperitoneal route as used in the present patient. Because hernia defects comprising colostomy and the lateral abdominal wall are too large to close, revision of colostomy seems most feasible, especially in the laparoscopic setting [7, 8].
In conclusion, gastric internal hernia associated with colostomy can occur as a rare complication. Although reduction of the incarcerated stomach is possible by nasogastric tube decompression, surgical repair of the hernia may be the optimal management to prevent the hernia recurrence.
CONFLICT OF INTEREST STATEMENT
We declare that there are no conflict of interests.
FUNDING
We declare that no funding was received in support of this work.

{kind=link}
{kind=link}