





Abstract
Spigelian hernia is a rare form of abdominal wall hernias. We report an unusual case of a strangulated spigelian hernia with necrotic contents of the caecum, appendix and terminal ileum in the elderly. An 84-year-old woman, with a history of eight pregnancies, was admitted for bowel obstruction evolving for 7 days. The computed tomography scan showed a strangulated right spigelian hernia. Surgical exploration with an incision centered on the mass confirmed the diagnosis with extensive necrosis of the caecum, appendix and 10 cm of the terminal ileum. A right hemi-colectomy with an ileo-colic anastomosis was performed. The post-operative course was marked by the death of the patient in intensive care due to multi-visceral failure. The occurrence of strangulation with necrosis of the caecum, appendix and terminal ileum in spigelian hernia is extremely rare. It requires early diagnosis and treatment to reduce post-operative morbidity and mortality.
INTRODUCTION
Spigelian hernia is defined by a passage of the abdominal organs through the parietal weak area of the same name. This area is located between the outer edge of the rectus muscle and the medial edge of the transverse abdominal muscle [1]. It is a rare form of abdominal wall hernias with a frequency between 0.1 and 2% [2]. Strangulation is a frequent complication in the evolution of this type of hernia, occurring between 17 and 40% of cases [3]. The most frequently contents are the small intestine and the omentum [4]. We report an unusual case of a strangulated spigelian hernia with necrotic contents of caecum, appendix and terminal ileum in an elderly woman.
CASE REPORT
An 84-year-old patient, gravida 8, para 8, consulted in emergency department for abdominal pain and vomiting evolving for 7 days. The blood pressure was 120/70 mm Hg with a fever at 38.6°. The physical examination found an ovoid non-reducible mass of the right lower quadrant (Fig. 1). There was no abdominal tenderness or peritoneal signs. The computed tomography (CT) scan showed a strangulated right spigelian hernia with a hernial ring measured to 3.4 cm. The content was the coecum (Fig. 2). There were also signs of bowel ischemia with pneumatosis and minimal peritoneal effusion (Fig. 3). Biology found leukocytosis at 15 200 elements per mm3. Surgical exploration with an incision centered on the mass confirmed the diagnosis. There was an extensive necrosis of the hernial sac and its contents (the caecum, appendix and 10 cm of the terminal ileum) (Figs 4 and 5). A right hemi-colectomy with an ileo-colic anastomosis was performed. The parietal defect was closed by an aponeurorraphy with Mersuture 0. The post-operative course was marked by the death of the patient in intensive care due to multi-visceral failure.

Non-reducible ovoid abdominal mass (arrow) of the right lower quadrant.
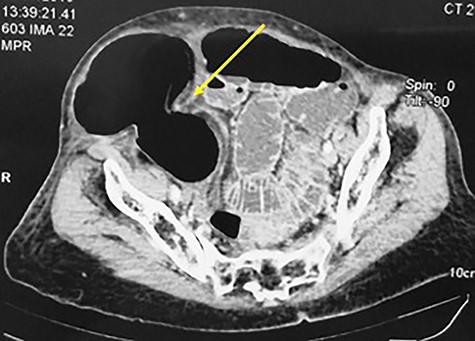
CT scan showing a strangulated right spigelian hernia with hernial ring (arrow) measured at 3.4 cm the coecum as content.

Abdominal CT scan showing a strangulated right spigelian hernia with pneumatosis (arrow).

Per operative view of the non-reducible spigelian hernia with necrosis of the sac.
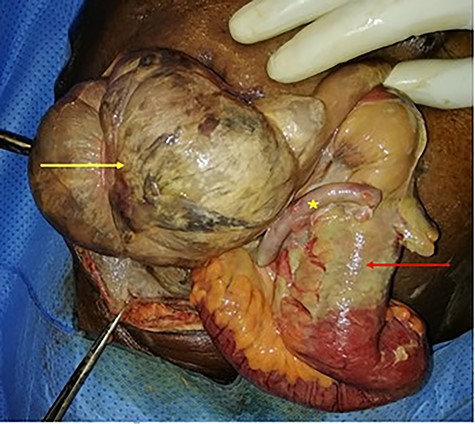
Per operative view of the contents with necrosis of the cecum (yellow arrow), appendix (star) and the terminal ileum (red arrow).
DISCUSSION
Spigelian hernia or interstitial ventral hernia was first described by Joseph Thaddaeus Klinkosh in 1764 [5]. It is named after Adriaan van den Spiegel who described the parietal weak area in the abdominal wall where this type of hernia occurs. This area is located between the lateral edge of the right muscles and the semi-lunar line (medial edge of the transverse muscles). The hernial ring is always a well-defined defect in the aponeurosis [6].
It is a rare form of abdominal wall hernias with an estimated frequency between 0.1 and 2% [2]. This type of hernia most often occurs below the umbilicus (90% of cases) in an area called the ‘Spangen belt’ [4]. This area is limited by the interspinous plane and a parallel line 6 cm above [5, 6].
Spigelian hernia is often acquired with age and rarely congenital [2]. Risk factors for intra-abdominal hyper pressure are often found such as obesity, chronic cough or ascites [4]. The predominance of women is noted in many studies. In the study of Malazgirt et al. [1], there were 88% women (30 women for 4 men). Women are more exposed with stretching in the abdominal wall caused by multiple pregnancies [6]. This could explain the occurrence in our patient who had eight pregnancies.
The relative rarity of spigelian hernia explains the diagnosis at the stage of strangulation. Indeed, spigelian hernia can remain asymptomatic for a long time. The swelling caused by the hernia is often small and goes unnoticed in the absence of complications [5]. The diagnosis at the strangulation stage is frequent, estimated between 17 and 40% of cases [3]. The risk of strangulation is higher because of sharp fascial margin around the defect [6].
Clinical presentation of strangulation depends on the existence of necrosis and hernia’s content. That content is more commonly the omentum or small intestine. Rarely, others organs as the appendix, colon or ovary can be found [7, 8]. In our case, we exceptionally found necrosis of the cecum, the appendix and 10 cm of terminal ileum.
Imaging remains essential in preoperative diagnosis. CT scan confirms the hernia and looks for signs of complications (pneumatosis, pneumoperitoneum). It also allows to measure the parietal defect and to determine the content of the hernial sac [2, 9]. The narrow hernial ring in our case (3.4 cm), determined on the CT scan, probably facilitated the occurrence of strangulation and necrosis.
The treatment for spigelian hernia is surgical. Laparoscopic approach with mesh seems to be the best option in the absence of complications [10]. It gives good results concerning post-operative pain, length of hospital stay and recurrence. In our patient, with the high risk of infection in the emergency context associated to intestinal necrosis, we opted for an open approach without mesh. Factors associated to the death of our patient were probably intestinal necrosis, consultation delay and the old age.
Spigelian hernia is a rare type of hernia. Strangulation is a complication that requires early diagnosis and treatment. Clinical presentation with necrosis of the cecum, the appendix and terminal ileum is exceptional. The laparoscopic approach with a mesh is the best option when there is no necrosis as it reduces post-operative morbidity and the risk of recurrence. However, in an emergency context, aponeurorraphy without mesh should be chosen to avoid the risk of infection.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}