





Abstract
Intestinal intussusception is a rare cause of intestinal obstruction; intestinal intussusception associated with endometriosis is very rare. The varied clinical presentations make the diagnosis demanding. In this article, we report the case of a young female patient with an intestinal obstruction due to intussusception. The successive histologic examination of the resected sample showed advanced endometriosis. This is a very rare entity with only a few similar cases reported in the literature.
INTRODUCTION
Intestinal intussusception is a rare cause of intestinal obstruction; intestinal intussusception associated with endometriosis, a chronic benign condition with a 10–20% incidence in reproductive-aged women, is very rare. A total of 3.8–37% of these patients manifests bowel endometriosis, and its pathogenesis is multifactorial [1, 2]. The varied clinical presentations make the diagnosis demanding.
CASE REPORT
A 32-year-old female patient presenting with vomiting and diarrhea associated with increasingly strong abdominal pain in the upper left quadrant in the last 24 hours was admitted to the emergency department. The patient reported constant abdominal pain and vomiting with diarrhea (four episodes/day) for 2 weeks. An initial conservative approach with oral analgesics, antibiotics and proton pump inhibitors by the general practitioner did not lead to any improvement in the patient’s condition. The patient’s last menstrual period was 2 weeks before and was unremarkable. The patient never had any such symptoms before.
In the anamnesis, an undefined open umbilical operation in childhood, probably due to an omphalocele, was reported. The rest of the anamnesis was unremarkable and without inflammatory bowel disease or colorectal cancer history in her family. No colonoscopy had been performed to date. The measured blood pressure and heart frequency were normal and the patient had no fever.
The clinical examination showed a slightly deteriorated condition and a painful distended abdomen with tenderness in all quadrants. There was no rebound pain or palpable masses. Blood tests showed a normal white cell count with a very slight elevation in C-reactive protein (7 mg/l). In the emergency department, the first diagnostic approach with ultrasonography revealed a circular concentric layer, with a maximum diameter of 4–5 cm, highly suspicious of invagination in the left upper quadrant (Fig. 1). The second step was to perform a CT scan with consequent confirmation of the diagnosis. The exam revealed a long ileocolonic intussusception of the ascending colon into the transverse colon, with possible involvement of the terminal ileum; a suspicious strangulation of a superior mesenteric artery branch was postulated (Figs 2 and 3).

Ultrasonography with a circular concentric layer highly suspicious of invagination.

CT scan with long ileocolonic intussusception of the ascending colon into the transverse colon, with possible involvement of the terminal ileum, coronal plane.

CT scan with long ileocolonic intussusception of the ascending colon into the transverse colon, with possible involvement of the terminal ileum, axial plane (white arrow).
The indication for emergency laparotomy followed. The inspection showed a massive ileocolic intussusception into the left side of the transverse colon. A reposition was not possible due to adhesions and bowel edema. An oncological extended right hemicolectomy was performed because of the unclear reason for intussusception (Fig. 4). The operation was successful with primary ileocolic anastomosis. The postoperative course was uneventful. Passage of gas occurred on the second postoperative day and passage of stool occurred on postoperative day four. Nine days after the operation, our patient was discharged from the hospital in very good condition.

Ileocolic specimen with endometriosis node as the cause of the intussusception.
The histological exam showed an ileocolic intussusception because of extended perimural adhesions in the range of severe local extended endometriosis with several foci in the lamina propria of the colon layer and in the fibrotic zone (Fig. 5).
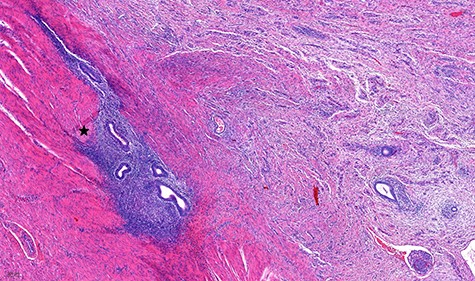
Histological specimen of the endometriosis (scale 200 μm). In detail the outer layer of the muscular bowel wall and adjacent subserosal tissue with fibrosis; embedded there are islands of inconspicuous endometrial-type glands and stroma (black star) with banal cytology.
Because of dysmenorrhea in the history, no further diagnostic was recommended, and contraception therapy was begun. At the 3-month follow-up, the patient was symptom-free.
DISCUSSION
According to the current literature, we present the 17th case of ileocolic intussusception due to endometriosis in a young female patient [3–6].
Endometriosis is a chronic benign condition with a 10–20% incidence in reproductive-aged women. A total of 3.8–37% of these patients manifests bowel endometriosis, and its pathogenesis is multifactorial [1, 2]. In the latter, the sigmoid colon and the rectum are the most frequently involved bowel parts [3]. The main symptoms are unspecific with abdominal pain, dysmenorrhea and dyspareunia. In cases of bowel involvement, the major symptoms could be cramping, dyschezia, cyclic rectal bleeding, diarrhea and obstipation. Bowel endometriosis could have an acute presentation with an acute abdomen and occlusion due to an intussusception, invagination and compression [1, 7, 8]. Although intussusception is a rare condition of bowel obstruction in adult patients, endometriosis should be considered a cause in every female patient of reproductive age [7, 9]. We recommend the use of CT scan for a proper diagnosis because of its accuracy of up to 90% [9]. After the correct diagnosis, a surgical approach is recommended in any case: conservative management to reduce the obstruction in cases of small bowel involvement; resection in cases where there is an inability to reduce the obstruction in the small bowel, in cases of suspected malignancy, or in cases of suspected large bowel involvement [10]. According to Nazif et al., and because reduction was impossible, we performed a primary resection with an extended right hemicolectomy [10].
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}