





Abstract
The number of robotic surgical procedures for thoracic disease is increasing. The automatic linear stapler has become a necessary device in endoscopic surgery. A 67-year-old man with a history of smoking was referred to our hospital for an abnormal finding on chest x-ray. Computer tomography of the chest revealed a ground glass nodule in the right middle lobe. We performed right middle wedge resection through the assistant port using a long-shaft stapler (LSS). Because the nodule was diagnosed as an adenocarcinoma on the intraoperative frozen section, the patient underwent robotic-assisted thoracoscopic surgery (RATS) right middle lobectomy using the da Vinci® Xi system. The pulmonary arteries, veins, right middle bronchus and minor fissure were divided using the LSS through the utility thoracotomy or assistant port. The postoperative course was uncomplicated. This case suggests that the LSS can be used in RATS lung resection for cancer.
Introduction
With technological advances, surgical approaches for thoracic diseases have shifted from thoracotomy to endoscopic surgeries such as video-assisted thoracoscopic surgery (VATS) and more recently, robotic-assisted thoracoscopic surgery (RATS). In 2009, the da Vinci® robotic surgical system (Intuitive Surgical, Sunnyvale, CA, USA) was released worldwide. The number of robotic surgical procedures for thoracic disease has been increasing ever since [1]. In endoscopic surgery, various automatic linear staplers are used, depending on the thickness, length, and location [2]. We report a case in which we had used a long-shaft stapler (LSS) in RATS, which is not popular in Japan, but particularly useful when moving from thoracoscopic lung biopsy to robotic lung resection for lung cancer.
Case Report
A 67-year-old man with a history of smoking was referred to our hospital for an abnormal finding on a chest x-ray. He had a history of left renal cancer, type 2 diabetes mellitus, hypertension and cerebral infarction.
His vital signs showed no abnormalities; the respiratory rate was 16 breaths per minute, and oxygen saturation was 97% on room air. Laboratory data revealed a serum hemoglobin A1c of 7.0%, serum carcinoembryonic antigen level 1.6 ng/ml (normal, below 5 ng/ml) and serum sialyl Lewis X-I antigen level of 27 U/ml (normal, below 38 U/ml).
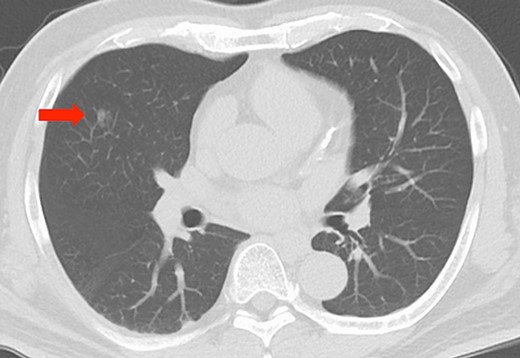
Imaging findings, chest computed tomography scan revealing a ground glass nodule, approximately 10 mm in diameter, in the right middle lobe (red arrow).
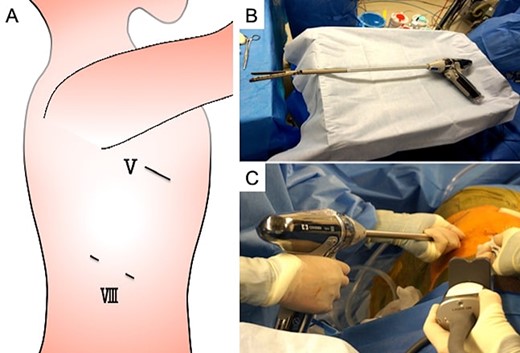
Thoracoscopic biopsy findings, (A) a 3-cm utility thoracotomy was performed at the fifth intercostal space (ICS) in the posterior axillary line. An 8-mm camera port and a 12-mm assisted port were placed at the eighth ICS in the middle axillary line and in the anterior axillary line, respectively. The line marked with ‘V’ indicates the fifth ICS; ‘VII,’ the eighth ICS. (B) The long-shaft stapler (LSS) attached with a Signia™ adapter XL (Covidien Japan, Tokyo, Japan) to the Signia™ Stapling System (Covidien Japan, Tokyo, Japan). (C) The nodule was removed via right middle wedge resection using the LSS from the assistant port at the eighth ICS.
Computed tomography (CT) of the chest revealed a ground glass nodule, approximately 10 mm in diameter, in the right middle lobe (Fig. 1).
Under general anesthesia, the patient was intubated with a double-lumen endotracheal tube and positioned in the left lateral decubitus position. Lung biopsy was performed for an accurate diagnosis. For palpating the nodule by finger, a 3-cm utility thoracotomy was performed at the fifth intercostal space (ICS) in the posterior axillary line, and a Gel POINT Mini Advanced Access Platform (Applied Medical, Rancho Santa Margarita, CA, USA) was placed. An 8-mm camera port and a 12-mm assisted port were placed at the eighth ICS in the middle axillary line and in the anterior axillary line, respectively (Fig. 2A). The nodule was removed via wedge resection of the right middle lobe using an LSS. The LSS was attached with a Signia™ adapter XL (Covidien Japan, Tokyo, Japan) to the Signia™ Stapling System (Covidien Japan, Tokyo, Japan) (Fig. 2B and C). After the nodule was diagnosed as an adenocarcinoma on intraoperative frozen section diagnosis, a 4-arm RATS right middle lobectomy was performed, leaving a 3-cm utility thoracotomy, using the da Vinci® Xi (Intuitive Surgical, Sunnyvale, CA, USA) (Fig. 3A). The pulmonary vessels, right middle bronchus and the minor fissure were divided using the LSS through the 12-mm port (Fig. 3B and C). The postoperative course was uncomplicated. Final pathological stage was stage IA1.
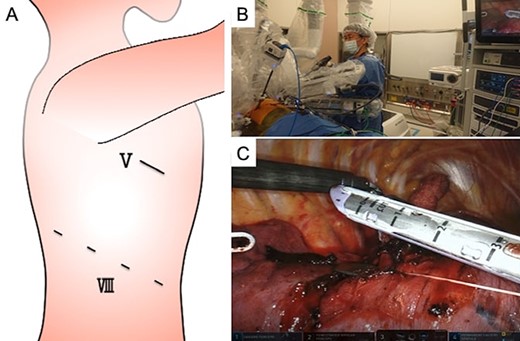
Robotic-assisted thoracoscopic surgery (RATS) findings, (A) a 4-arm RATS right middle lobectomy was performed, leaving a 3-cm utility thoracotomy, using the da Vinci® Xi (Intuitive Surgical, Sunnyvale, CA, USA). The line marked with ‘V’ indicates the fifth intercostal space (ICS); ‘VII,’ the eighth ICS. (B) An assistant used the long-shaft stapler (LSS) (Signia™ stapling system with Signia™ linear adaptor XL, Covidien Japan, Tokyo, Japan) from the utility thoracotomy during RATS lung resection. (C) The fissure between the right upper and middle lobe was divided from the utility thoracotomy using the LSS.
Discussion
The number of robotic surgical procedures is increasing worldwide [1]. Recently, progress in both imaging techniques and diagnoses has allowed the detection of early stage lung cancer. To make definite diagnoses, various procedures are performed, including bronchoscopic and thoracoscopic biopsy. If the tumor is determined to be malignant, VATS lung resection can be performed subsequently. When national health insurance began to cover RATS for malignant lung tumors, malignant mediastinal tumors and benign mediastinal tumors in Japan starting in 2018, the number of domestic RATS performed domestically has increased rapidly [1].
Since 2013, we have been performing RATS lung resection for resectable malignant lung diseases. We perform RATS lobectomy using the da Vinci® S and Si (Intuitive Surgical, Sunnyvale, CA, USA) with four port incisions utilizing a 3-cm utility thoracotomy. The assistant stands at the anterior side of the patient, assisting through the utility thoracotomy by providing additional retraction of the lung and suction when necessary, and using a port to perform the stapling. Since 2018, we have been performing RATS lobectomy using da Vinci® Xi with four port incisions and carbon dioxide insufflation combined with an assistant port or a 3-cm utility thoracotomy. Especially, as thoracoscopic biopsy recommend for undiagnosed lung nodules, it is necessary to place the port arrangement anticipating RATS lung resection. Therefore, the two ports are placed in the same eighth ICS, and a 3-cm utility thoracotomy due to palpating the nodule by finger is added to the fourth or fifth ICS for the thoracoscopic lung biopsy. Because the assistant uses the stapler from the port, the distance to the target area increases. When it is converted from the thoracoscopic procedure to RATS for malignant lung diseases, the utility thoracotomy is often hidden by the robot arm, and all ports placed in the eighth intercostal space are far from the target area. Furthermore, the assistant working space outside the patient’s body is limited by the robot arms. Although a robotic stapler is easy to use, it is more expensive than conventional endoscopic staplers [3, 4]. The cost can be reduced by using the stapler system used for thoracoscopic biopsy. Many thoracic surgeons are familiar with endoscopic staplers that have many variations. Not widely used in Japanese thoracic surgeons, the Signia™ stapling system (Covidien Japan, Tokyo, Japan) has an adapter to extend the shaft. By attaching an adapter, the shaft can be extended by 10 cm. This permits easy handling of the LSS (Signia™ stapling system with Signia™ linear adaptor XL, Covidien Japan, Tokyo, Japan) during both thoracoscopic biopsy and RATS lung resection.
Our case demonstrates that LSS can be used in RATS lung resection after thoracoscopic lung biopsy.
Funding
Not applicable.
Conflict of interest statement
The authors declare that they have no competing interests.
Authors’ contributions
S.M. drafted the manuscript. M.K. performed the surgery. H.M. and T.I. assisted in performing the surgery. M.K. critically revised the manuscript. All authors have read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
The patient consented to publication of this case.
Availability of data and materials
All the data and materials supporting our findings are included within the article.
ACKNOWLEDGEMENTS
Not applicable.

{kind=link}
{kind=link}
{kind=link}