





Abstract
Gallbladder cancer (GBC) is a rare disease characterized by its aggressiveness. Resection with free tumour margins is the sole curative treatment and, in incidental findings, surgical reapproach is recommended for segmentectomy IVb and V or wedge resection of the gallbladder fossa and lymphadenectomy. Here we report a case of gallbladder adenocarcinoma as an incidental finding in a fragment in its lumen with no wall involvement evidentiated. The patient was reoperated for resection of the gallbladder bed with hepatic hilum and cystic duct lymphadenectomy, later evidentiated as free of residual disease. The normality of the bile ducts evidenced by imaging studies, in addition to signs of chronic cholecystitis corroborate to GBC diagnosis. We suspect that the fragment was detached gallbladder polypoid neoplastic lesion. Despite the lack of clinical manifestations, the fast surgical interventions and the histopathological analysis of the material was probably a prognostic determinant for the patient.
INTRODUCTION
Gallbladder cancer (GBC) is the most common neoplasm of the biliary tract, with low incidence worldwide, especially in western countries. Inconspicuous and ill-defined symptomatology, together with the aggressiveness of the disease, gives GBC high mortality rates and restricted overall survival [1]. GBC is most frequently diagnosed incidentally after cholecystectomy for suspected benign disease, a situation in which surgical reapproach is advisable [2–4]. Surgery is the only curative treatment and should be associated with adjuvant therapy in more advanced cases [5, 6]. Here we report a case of gallbladder adenocarcinoma as an incidental finding in a fragment in its lumen without wall involvement.
CASE REPORT
The patient was a male 43 years old, with a medical history of prediabetes, overweight, 20-pack-year smoking and maternal history of biliary tract cancer at 63 years. He denied any gastrointestinal symptoms at the time. In April 2018, during follow-up for nephroureterolithiasis, the patient’s abdominal computed tomography (CT) showed multiple hypoattenuating round masses compatible with calculous cholecystopathy and 1.3 cm hyperattenuating content.
The complementary ultrasound revealed no gallbladder alterations besides several calculi. He underwent cholecystectomy in June 2018, which histopathological material evidenced signs of chronic calculous cholecystitis with foci of low-grade epithelial dysplasia and a well-differentiated tubular adenocarcinoma loose fragment permeating smooth muscle tissue. The immunohistochemistry of the fragment revealed adenocarcinoma possibly from the biliary tract.
Staging exams were performed and showed no signs of metastatic disease. At the magnetic resonance cholangiography, there was no obstruction or filling defects of intra or extrahepatic, common and pancreatic bile ducts; and no expansive lesions or collections along with the surgical topography. The values of serum tumour markers carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA) and alpha-fetoprotein were 292.4 U/ml, 2.3 ng/ml and 3.3 ng/ml, respectively. Bilirubin and glutamic oxaloacetic transaminase levels were regular.
In October 2018, the patient underwent laparotomy for resection of the gallbladder fossa and dissection of the cystic duct and hepatic hilar lymph nodes (Fig. 1a and b). The anatomopathological analysis revealed no residual neoplasia, with six lymph nodes free of neoplasia. The patient is still in follow-up and is free of disease. The patient consented for publication of this case report.
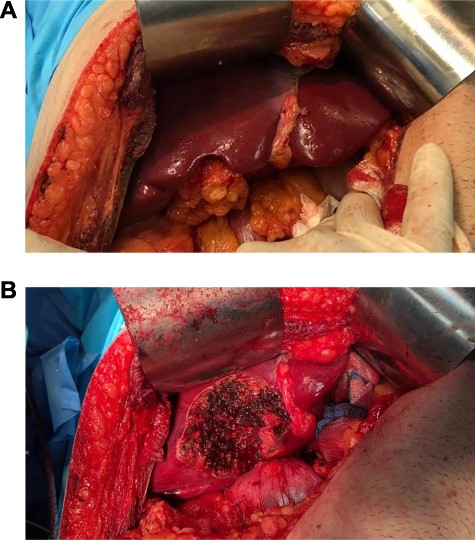
Intraoperative photograph before (a) and after (b) resection of the gallbladder fossa and lymphadenectomy.
DISCUSSION
GBC is rare in western countries with an estimated worldwide incidence of 2/100,000, higher in developing countries [1]. This disease is characterized by its aggressiveness [5]. Overall 5-year survival ranges from 5 to 32% and only 10% are diagnosed while restricted to the gallbladder [2, 7, 8]. The average survival of patients with advanced GBC is <6 months and three-fourths of patients die within a 1 year [7, 9]
The female-to-male incidence rate ratio reaches 3:1 [1, 2, 7], which is related to the higher rates of biliary lithiasis in women due to oestrogen influence. Cholelithiasis is considered a major risk factor for GBC and its pathophysiology is related to the consequent chronic cholecystitis. Along with exposure to other carcinogens, this chronic inflammation leads to metaplasia, followed by dysplasia and the development of carcinoma in situ, in a process that lasts ~15 years. This pathophysiological hypothesis is corroborated by the fact that 90% of patients with GBC have dysplasia and carcinoma in situ and on account of most cancers being adenocarcinomas, as presented in this case [1, 2].
Other risk factors are: obesity, smoking, excessive fried food intake and regular exposure to biofuels. Fruit and vegetable consumption is considered a protective factor [1, 2, 7]. A familial association has been described in 26% of cases, denoting the genetic susceptibility to GBC, in which maternal transmission has been predominant [2]. Early lesions may present as a mucosal plaque, polypoid or papillary projection and the symptoms of GBC are inconspicuous [1, 2]. The tumour markers mostly used in this scenario and the levels that suggest a diagnosis of GBC are CEA, when >4 ng/dl and CA 19–9, in levels >20 ng/dl, with low specificity [1].
Resection with free tumour margins is essential to treatment. Radical resection must be performed in most cases and can be either segmentectomy IVb and V or wedge resection of the gallbladder fossa and no evidence of difference between the techniques [8]. Lymph node involvement is the most relevant prognostic factor [8, 10]. For an adequate lymphadenectomy, a minimum of 6 regional lymph nodes should be resected, mostly from the hepatoduodenal ligament. A prospective study showed that around 20% of tumours are inoperable at diagnosis, with 70% of these having peritoneal involvement, suggesting the potential value of staging laparoscopies in GBC [10].
The use of neoadjuvant therapy has not yet been established as a standard approach [2, 10]. Adjuvant treatment is recommended for stages II or above, margins or positive lymph nodes [10]. The drugs used in chemotherapy are gemcitabine, cisplatin and 5-fluorouracil [6]. Adjuvant radiotherapy reduces local recurrence rates and increases short-term survival when associated with chemotherapy [3, 6].
Incidental findings of GBC amount to almost 80% of diagnoses [3]. Histopathological verification of malignancy occurs in 6–15% of patients who underwent cholecystectomy for cholecystolithiasis [4]. In these cases, in tumours with stages T1b or above, surgical reapproach for extended resection is recommended. In one study, residual disease was found in 74% of cases, with a high recurrence rate, with the majority (75%) occurring at distant sites [3].
In our case, the presentation of GBC as a fragment in the content of the gallbladder also raised the diagnostic suspicion of another type of bile duct neoplasm that could have detached and be carried to the lumen. However, the normality of the bile ducts evidenced by imaging studies, in addition to signs of chronic cholecystitis corroborate to this diagnosis. We suspect that the fragment was detached gallbladder polypoid neoplastic lesion, which could be the hyperattenuating image showed in the patient’s CT. Despite the lack of clinical manifestations, the fast surgical interventions and the histopathological analysis of the material was probably a prognostic determinant for the patient.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest relevant to this manuscript.
FUNDING
None to declare.

{kind=link}