





Abstract
Inguinal hernia is a common general surgery presentation. Large inguinoscrotal hernias can contain large bowel, omentum, small bowel, Meckel’s diverticulum but rarely ureter and bladder. Ultrasound can further clarify contents of inguinal hernia, and for this patient, it showed a cystic structure in the hernia contents. This was further investigated and found to be the left ureter with moderate to severe hydronephrosis. The patient underwent left inguinal hernia repair without any complication because of the anticipated anatomical anomaly. This case is to raise awareness that a simple inguinoscrotal hernia repair could be complicated by ureteric injury if not investigated thoroughly in the preoperative stage.
INTRODUCTION
Ureteral hernia was first described in 1880 and <140 cases have been reported in the literature ever and even fewer described with incarceration and ureteric obstruction [1, 2]. Ureteral inguinal hernia is more common in male and more so in their fifth or sixth decades of life. It is quite common with patients with history of renal transplantation. Most patients are asymptomatic, and the findings are picked up as incidental finding on radiological investigation. We report a rare presentation of ureter in left inguinal hernia in an elderly obese male.
CASE REPORT
We present an 84-year-old male who presented to Emergency Department from his General Practitioner with ultrasound showing cystic structure in large inguinoscrotal hernia. He has a past medical history of ischemic heart disease, reflux disease, hyperlipidaemia, obesity, appendicectomy and cholecystectomy.
He was complaining 3 months of bilateral scrotal pain and swelling but worsening in the last 2 weeks. Computed tomography (CT) of abdomen/pelvis was performed to further investigate cystic structure in the inguinoscrotal hernia. It was reported as large left inguinoscrotal hernia containing left ureter with moderate to severe hydronephrosis and mild inferior lateral traction on right ureter (Figure 1a, 1b and 1c). Patient did not present with any bowel obstruction symptoms. Initial blood test was unremarkable with Wcc 6 × 109/L, CRP 3, Urea 6.4 mmol/L and Cr 75 umol/L.
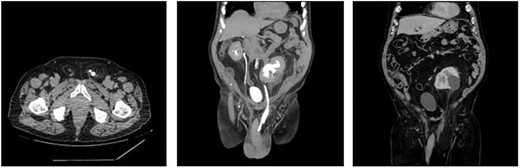
(a) Axial view of CT urogram showing left ureter folding on itself in the left inguinal canal. (b) Coronal view of CT urogram showing moderate-to-severe hydronephrosis and hydroureter of left kidney. (c) Coronal view of CT abdomen-pelvis showing peritoneal contents pulled into the large left inguinoscrotal hernia.
He was consented to have bilateral open inguinal hernia repair. The left side inguinal repair was carefully dissected, and ureter was clearly identified and separated from vas deferens. The hernia was repair with a traditional Lichtenstein approach with Ultra-pro mesh. The patient was kept as inpatient for 2 days for analgesia and observation. He was discharged and had complete recovery after his surgery.
DISCUSSION
Large inguinoscrotal hernia often contains multiple peritoneal contents, but ureter is one of the rare retroperitoneal structures that herniate through. Herniation of the ureter can occur not only through the inguinal canal, but also through femoral ring, sciatic foramen and even diaphragm [3]. Ureter herniation found more in indirect hernia vs direct hernia (80% vs 20%).
Two anatomical variants are found: paraperitoneal and extraperitoneal. Paraperitoneal type occurs more commonly (80%), where its peritoneal indirect sac pulls the ureter and forms part of the hernia. Less commonly the extraperitoneal type occurs without a peritoneal sac, where there is large amount of peritoneal fat, which slides down and contains the ureter [4]. The retroperitoneal structures prolapse downwards to form a sliding hernia.
Routinely patients do not warrant any imaging for large inguinal hernia. In the setting of large inguinoscrotal hernia where a variety of organs can herniate through, it is crucial to have adequate preoperative assessment with radiological guidance. Any suspicion of urological organ involvement warrants CT urogram for preoperative planning [5]. This serves as a reminder to the surgeon to be mindful of structures during the dissection. In this case, the ureter was clearly identified and reduced. Anatomy can be confusing during a large inguinoscrotal hernia repair where it might contain omentum, small bowel, large bowel, bladder and retroperitoneal structures. The surgeon will need to proceed with caution during dissection and avoid ligation/injury to the herniated organs. This case report will raise awareness that a simple inguinoscrotal hernia repair can be complicated with ureteric injury if inadequate preoperative assessment was performed and the surgeon not aware of ureteric involvement.

{kind=link}