





Abstract
Although parastomal hernias are a common complication of ostomy formation, herniation of intra-abdominal organs, aside from intestine, is infrequent. Furthermore, herniation of retroperitoneal organs, such as the kidney, is an extremely rare finding. We report the case of a 59-year-old male with a right ileostomy who presented with an acute kidney injury with suggestive urinary tract infection. A computed tomography scan revealed a left proximal ureteral stone with left hydronephrosis and a prominent right parastomal hernia with herniation of the mesenteric/retroperitoneal fat, portion of the right kidney, right proximal ureter and some bowel. The patient was taken to the operating room for a left cystourethroscopy with stent placement and made a full recovery. Due to the patient’s extensive surgical history, high risk of postoperative infection and lack of evidence demonstrating functional impairment of the right kidney, surgical intervention was not recommended at the present time.
INTRODUCTION
A parastomal hernia is an incisional hernia that allows protrusion of intra-abdominal contents, most commonly fat, mesentery or intestine, through a surgically created abdominal wall defect. It is a very common complication of ostomy construction and can occur up to 48% following end-colostomy formation and 28% following end-ileostomy formation. Patient-specific risk factors for parastomal hernia formation include obesity, weight gain after ostomy construction, advanced age, wound infection, malnutrition and malignancy. Technical risk factors, such as the diameter of the abdominal wall defect, open versus laparoscopic technique for ostomy formation and emergent ostomy construction—also influence the rate of parastomal hernia formation.
Most patients with parastomal hernias are asymptomatic, but common symptoms are abdominal discomfort or pain and a bulge at the site of the stoma, or adjacent to it. Due to the high rate of recurrence, conservative management is recommended for patients with parastomal hernias who do not have acute complications or chronic symptoms that impair their quality of life. Surgical repair is warranted for patients with life-threatening complications or chronic bothersome symptoms [1].
We report a case of an adult male with parastomal hernia formation with right kidney herniation following the end-ileostomy construction.
CASE REPORT
A 59-year-old male with a past medical history of paroxysmal atrial fibrillation and class III obesity presented to the emergency department with complaints of intermittent palpitations for the past 2 weeks, increased watery output from his ileostomy and worsening bilateral lower extremity edema. He denied chest pain, diaphoresis, shortness of breath, dizziness, nausea, vomiting and abdominal pain. On physical examination, he was not in acute distress. He was tachycardic with sinus rhythm and his remaining vitals were stable. Abdominal exam demonstrated a large midline abdominal scar and a right ileostomy. The ileostomy was positive for watery stool. The bilateral lower extremities demonstrated 4+ edema. The rest of the physical exam was unremarkable.
The patient’s past surgical history is very complicated. In February 2015, the patient presented for ischemic colitis with bowel perforation, requiring an exploratory laparotomy that resulted in a subtotal colectomy with end ileostomy. His hospital course was protracted due to wound infections and intra-abdominal abscesses. After 7 months, he presented for an ileostomy reversal and underwent a laparotomy with small bowel resection and ileocolic anastomosis. His hospital course was protracted once again due to an intra-abdominal anastomotic leak and multiple abdominopelvic abscesses. This resulted in a resection of his ileoproctostomy, multiple abdominal washouts, a small bowel resection and creation of an end-ileostomy. In 2016, the patient presented multiple times with a recurrent left retroperitoneal abscess along the posterior abdominal wall and underwent three open abdominal surgeries for incision and drainage. A computed tomography (CT) scan from November 2016 did not show any evidence of kidney herniation (Fig. 1).

Computed tomography (CT) image from 2016 shows the right kidney in normal anatomical position.
Laboratory values showed evidence of an acute kidney injury with suggestive urinary tract infection. Renal ultrasound demonstrated bilateral nephrolithiasis with moderate left hydronephrosis. Abdominal/pelvic CT scan confirmed left proximal ureteral stone with left hydronephrosis and a prominent parastomal hernia at the ileostomy site, which contained portions of the right kidney, right proximal ureter, mesenteric/retroperitoneal fat and some bowel (Fig. 2).
The patient was taken to the operating room for a left cystourethroscopy with stent placement. Due to the patient’s extensive surgical history—high risk of surgical complications—and lack of evidence indicating right renal impairment, ileostomy revision and parastomal hernia repair with relocation of the right kidney was not recommended at this time.
DISCUSSION
Kidney herniation is very uncommon with only a few case reports of congenital herniation, traumatic thoracic herniation, postoperative renal transplant herniation and one report of postoperative incisional herniation [2–5]. In this case report, we discuss the first reported case of partial kidney herniation into a parastomal hernia.
Parastomal hernia is the most common complication of ileostomy and colostomy. Usually, only mobile structures, such as the small intestine and omentum, herniate into parastomal hernias. The kidney is normally firmly anchored in the retroperitoneum by the fascia and overlying peritoneum. We do not know what mechanism allowed for kidney herniation in this patient. We hypothesize that the recurrent retroperitoneal abscesses and mechanical forces, such as obesity and recurrent surgeries, might have played a role. At this time, there is not any evidence of functional impairment of the right kidney, and surgical intervention is not warranted. The patient will continue to be followed closely for evidence of any complications.
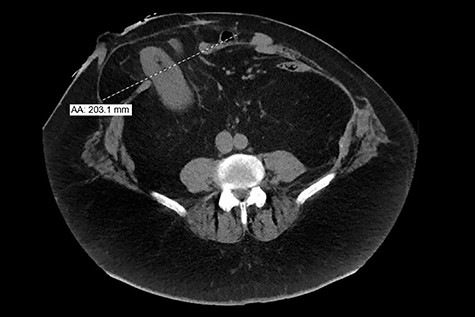
CT image from 2019 shows a prominent (2.3 cm ML) ventral hernia at the ostomy site, including portions of mesenteric/retroperitoneal fat, portion of right kidney, right proximal ureter and some bowel.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}