





Abstract
We describe a case of a middle-aged female who was diagnosed with synchronous primary lung and breast cancer following a bout of recurrent chest infections. Subsequent Multi Disciplinary Team (MDT) discussion proposed that in light of the patients’ multiple comorbidities, both lesions should be resected simultaneously under one general anaesthetic. The patient underwent an initial left mastectomy and axillary node clearance. Through the same incision, a left anterolateral thoracotomy was created to complete a left lower lobectomy. Post-operatively she made an uncomplicated recovery and was discharged 7 days after the procedure. Despite undergoing a longer and more complex procedure, her length of stay was in keeping with the average length of stay for a patient undergoing a thoracotomy and lobectomy [1].
This case highlights the importance of a pre-planned multidisciplinary approach to deal with synchronous pathology in an efficiently synchronous manner to improve patient outcomes.
INTRODUCTION
Ductal carcinoma in situ (DCIS) is a heterogeneous, unicentric precursor of invasive breast cancer [2]. Mastectomy is the best available treatment in achieving long-term cure. The gold standard operation for resectable early-stage non–small-cell lung cancer is in the form of a lobectomy, either via a video-assisted thoracoscopic surgery (VATS) or thoracotomy approach. We present a never-described before case of removal of synchronous primary breast and lung cancers via a single incision approach with a positive outcome.
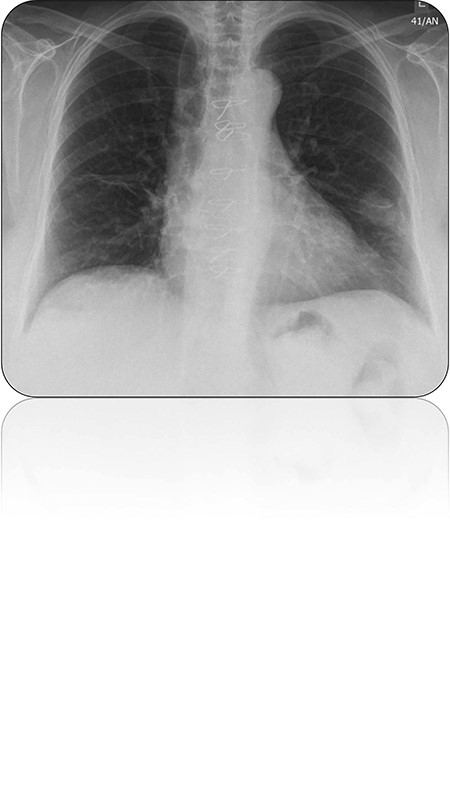
Chest radiograph demonstrating left lower lobe lesion.
CASE REPORT
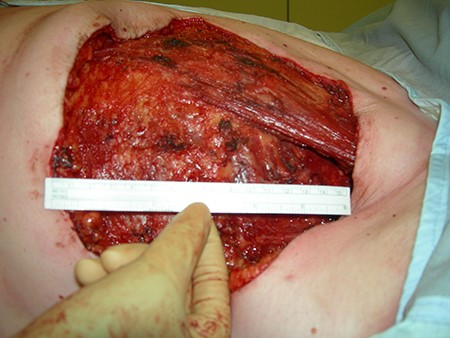
We describe a case of a middle-aged female diagnosed with synchronous primary lung and breast cancers. A history of recurrent chest infections resulted in the request of a routine chest X-ray. This subsequently demonstrated a nodule within the left lower lobe (Fig. 1). Computer tomography (CT) of the thorax demonstrated a mass within the left lower lobe as well as enlarged axillary lymph nodes. Previous mammography and magnetic resonance imaging had failed to demonstrate any lesions within the left breast. The aforementioned was further evaluated by positron emission tomography with CT, which demonstrated the lung lesion and lymph nodes to be metabolically active. Comorbidities included an aortic valve bioprosthesis, osteoarthritis, fibromyalgia and multiple gynaecological operative procedures. Biopsy of an axillary lymph node proved to be of breast origin. A CT-guided biopsy of the lung lesion demonstrated it to be of primary lung origin. This case was discussed at the multidisciplinary meeting and it was decided that this patient is a candidate for surgery to remove both lesions. This patient was subsequently brought forth for concomitant surgery to remove both the breast and lung lesions. Initially patient underwent a left mastectomy (Fig. 2) and left axillary node clearance. Attention was then directed towards completing a left lower lobectomy via an anterolateral thoracotomy through the same mastectomy incision with the patient supine but tilted towards the right (Fig. 3). Post-operative recovery was essentially unremarkable and the patient was discharged 1 week following her procedure. Histology was consistent with both primary adenocarcinoma of the lung and metastatic breast carcinoma within the lymph nodes and a ductal carcinoma in situ arising from the left breast (Fig. 4). The patient was subsequently referred for further oncological therapy.
Mastectomy.

Thoracotomy through the original mastectomy incision.
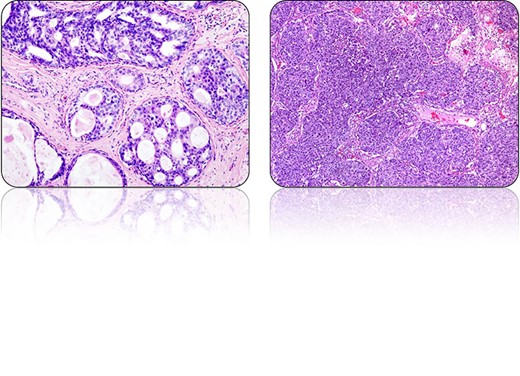
The characteristic histological appearances of (left) DCIS and (right) lung adenocarcinoma.
DISCUSSION
Within the current literature, there are case reports describing patients with synchronous tumours including combined operative and stereotactic oncological procedures with favourable outcomes [3]. We describe a novel, pre-planned multidisciplinary approach to deal with dual pathology leading to a favourable outcome and potentially decreasing post-operative morbidity by limiting number of incisions and it is likely to reduce combined operative stress in comparison to individual procedures and result in a faster post-operative recovery with less pain, and a reduced inpatient length of stay. Furthermore, the anterolateral thoracotomy through the pre-existing mastectomy incision provides sparing of the latissimus dorsi muscles, which could be used for reconstructive purposes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}