





Abstract
Following an uneventful arthroscopic menisectomy of the right knee, a white circular skin lesion, 1 cm in diameter, was noted on the anterior left thigh of a 23-year-old patient. The overlying paper surgical drape had not ignited nor produced smoke. Close inspection revealed a minute perforation in the drape with slight discolouration. No electro-cautery, radio-ablation or irritant skin preparation had been used during surgery. Tests failed to identify fault with the light source, fibre-optic cable or arthroscope.
The lesion was diagnosed as a full-thickness thermal burn resulting from heat transmitted from a 300-W Xenon lamp via a detached fibre-optic cable. The effects of contact between an illuminated fibre-optic light cable and living human skin are described, with changes in appearances followed over 2 years. Patients may be burnt and permanently scarred without the knowledge of staff in operating theatres if detached light cables rest against surgical drapes.
INTRODUCTION
More than 100 000 knee arthroscopies are performed annually in the UK [1].
Arthroscopy uses intensely white light, transmitted along a fibre-optic cable, to illuminate the joint cavity. Xenon arc lamps, with a bulb power of 300 W, are commonly used light sources.
Possible causes of skin burns in operating theatres include inadvertent electric discharge, irritant skin preparations, direct pressure and thermal necrosis induced by heated irrigation fluid or high-intensity light.
Cutaneous burns sustained by patients during knee arthroscopy are rare. A national review from the UK identified only seven cases over 15 years, a period when some 50 000 knee arthroscopies were performed annually in the UK [2, 3].
CASE REPORT
An arthroscopy of the right knee was undertaken on a 23-year-old man for a symptomatic lateral meniscal tear. Surgery was uneventful and was performed by an experienced surgeon and scrub nurse.
Upon removal of the paper surgical drapes, a circular and white lesion with an inflamed periphery measuring about 1 cm in diameter was noted on the patient’s anterior left thigh (Fig. 1a). Examination of the surgical drape revealed a pin-hole sized perforation with localized brown staining on the part that had covered the left thigh.
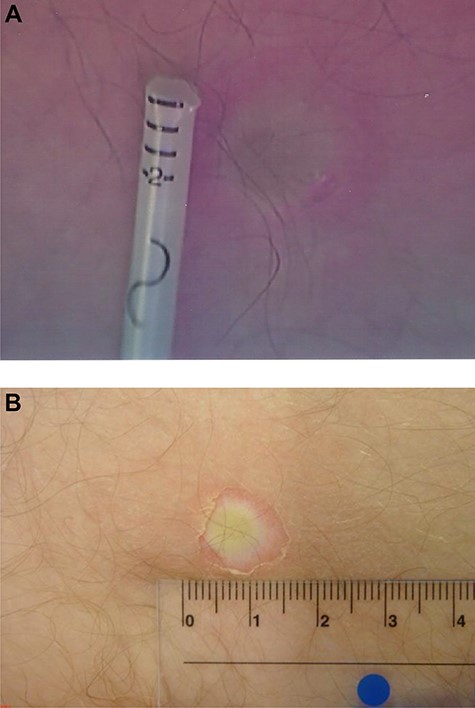
Patient’s burn within 2 hours of surgery. (a) In theatre (mm scale). (b) On ward (numbers in cm).
During surgery, the arthroscopic stack (Dyonics 300XL, 300-W bulb, Smith and Nephew, Andover, MA, USA) had been placed on the left side of the patient, beside the scrub nurse. The surgeon had stood on the patient’s right side throughout. The fibre-optic cable (5 mm, Gemini) had trailed across the front of the patient’s left thigh above a paper surgical drape (Mölnlycke, Swe). The light cable had been attached to the 4-mm diameter arthroscope via an adaptor (Versitip 2141, diameter 1.2 cm) with the light source switched off at the start of the operation. Following illumination the arthroscope had been inserted into the knee without delay. The light source had been on for ~50 minutes. There had been no evidence of smoke or burning. Neither electro-cautery nor radio-ablation had been used during the operation and there was no metallic contact to discharge electricity via the left thigh. A non-alcoholic skin preparation containing iodine had been used on the right lower limb only.
Upon discharge from hospital on the same day as surgery (Fig. 1b), the patient was referred to a plastic surgeon who diagnosed a full-thickness burn and advised non-operative management. The hospital sent the arthroscopic stack and illumination system for testing. No fault was found.
The orthopaedic surgeon reviewed the patient’s burn 6 weeks after operation (Fig. 2). The lesion was painful and took months to heal.

Patient’s burn 6 weeks following surgery.
In order to learn more about the cause of the burn, the surgeon experimented on himself.
With the 300-W Xenon light source set on average brightness, he applied the illuminated tip of the arthroscope and illuminated end of the light cable with adaptor, alternately to his left calf for periods of 10 minutes each (Fig. 3). He also applied the illuminated light cable and adaptor with the paper drape intervening for 10 minutes. During these tests, undertaken in the first 30 minutes of illumination, no pain was experienced and the paper was unblemished.

Illuminated fibre-optic cable end with attached adaptor (left) alongside unilluminated arthroscope connected to another cable (right).
In the second 30 minutes of testing, the brightness setting was raised to maximum and 10-minute applications repeated. Within 20 minutes of the light source being on, the cable end was too hot to hold against the skin for >45 seconds. A small white mark was evident on the skin within a minute of application (Fig. 4). Testing with the intervening drape at this stage produced a small burnt perforation in the paper without visible smoke (Fig. 5). Within 4 hours, blisters appeared on the surgeon’s calf even at points that were not initially blemished following contact with the cable adaptor or the arthroscope end (Fig. 6). The burn marks on the calf became more inflamed over the first 6 weeks. Lesions resulting from the fibre-optic cable were wider than those caused by the arthroscope tip and also formed a central scab. Scars remained inflamed for about 6 months. Burns faded significantly by 2 years (Figs 7–9).

Surgeon’s calf immediately following test.

Burn mark on paper drape from test.

Blistering on surgeon’s calf 4 hours after test.

Two weeks after test.

Six weeks after test. The larger scabbed lesions are a result of applying the light lead directly, whereas the smaller lesions result from application of the arthroscope tip.

Two years after test.
DISCUSSION
In this case the patient’s burn had a diameter and pattern matching that created by the direct application of the illuminated light cable and adaptor to the surgeon’s skin. Self-experimentation suggests the burn likely developed at the end of the procedure, by inadvertent approximation of the cable to the drape overlying the patient’s thigh. The diameter of the burn suggested it could not have arisen from the tip of an illuminated arthroscope.
The most troubling aspect of this case is that the patient was burnt without the surgical team being aware.
In vitro tests by Sandhu et al. recorded a temperature of 42°C at the tip of the active arthroscope and a temperature of 101°C at the end of a light lead illuminated by a 300-W Xenon lamp [4]. They found that the light lead was capable of thermal burning within seconds with combustion most likely if the light cable end was held some 0.5 cm away from the drape.
Spradling et al. determined that illuminated cables burnt cadaveric skin without damage to overlying drapes, whereas illuminated rigid endoscopes did not cause injury [5].
Despite the prevalence of knee arthroscopy, only one previous report of a thermal burn to the lower limb from a light cable was traced on literature review [6]. In that study, surgeons were alerted by smoke from drapes burnt by a fibre-optic light lead. The appearance of the underlying skin burn in that study is strikingly similar to those documented in this report. It should be noted that modern surgical drapes, made mostly of non-woven polypropylene, do not readily support combustion in room air [7].
The lesson from this case report is clear: even momentary proximity between an illuminated arthroscopic light lead and a surgical drape can cause a full-thickness burn to the patient’s skin without generating any smoke or fire. The risk of thermal injury rises with the brightness of the lamp used.
Light sources must be switched off prior to detachment of the light cable and adaptor from the arthroscope.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}