





Abstract
This is the case of a 27-year-old female who underwent breast lumpectomy for fibroadenoma of the left breast. Pathologic evaluation of the specimen revealed lobular carcinoma in situ (LCIS) entirely confined to a large fibroadenoma without LCIS in the surrounding breast tissue.
INTRODUCTION
Fibroadenoma is the most common solid mass diagnosed in the breast. The peak incidence is in the second and third decade. Histologically, fibroadenomas consist of a stromal and epithelial component. Fibroadenomas may be classified into simple and complex. Complex fibroadenomas are described as having cysts >3 mm in size, sclerosing adenosis, epithelial calcifications or papillary apocrine changes [1]. Radiologically, fibroadenomas appear as a slightly lobulated, homogenous, isoechoic or hypoechoic solid mass [2].
Typically considered a benign tumor, reports exist of both invasive and in situ neoplasms being found within the fibroadenoma. The radiographic changes of a neoplasm in a fibroadenoma are subtle focal increases in color flow signals on Doppler ultrasound [2]. Within a screened population, the incidence of carcinoma within a fibroadenoma is 0.1–0.3% [3,4]. Because of the low frequency, these specimens are typically found after a lumpectomy for expected benign disease.
Lobular carcinoma in situ (LCIS) is a neoplastic proliferation of the epithelial cells of the breast lobule. Originally, this was considered a pre-cancer to invasive lobular carcinoma, similar to the relationship between ductal carcinoma in situ and invasive ductal carcinoma. However, LCIS is now considered a general marker for breast cancer risk, rather than a true pre-cancer. Wu et al. challenged this and found that LCIS within a fibroadenoma is associated with invasive breast cancer [5].The incidence of LCIS within a fibroadenoma is rare and estimated to be about 17% of neoplasms found within a fibroadenoma. It has been estimated that neoplasms found within fibroadenoma behave in a similar fashion and carry the same prognosis as those found independently. We present here a case of a young female found to have LCIS within a fibroadenoma.
CASE REPORT
A healthy 27-year-old female with a history of fibrocystic breast disease presented with chief complaint of an enlarging painful lump in the outer portion of the left breast. The lump had been present for 4 months. She also admitted to a second mass behind her nipple that had been present for 3 years. The retroareolar mass was previously biopsied, determined to be benign, and had not changed since initial presentation. She complained of worsening pain at the outer mass due to friction from the seat belt.
Upon physical exam, she was found to have a palpable mass of the upper outer quadrant of the left breast that was freely mobile and firm. She had a second palpable mass in the retroareolar region at the 2 o’clock position that was slightly smaller. This mass was firm and mobile. 3D digital breast tomosynthesis mammography demonstrated a mass within the retroareolar region of the breast and a mass within the upper outer quadrant of the breast posteriorly. No asymmetric breast mass was seen on the right side. No micro-calcifications were evident on either side. Left breast ultrasound revealed a heterogeneous hypoechoic solid mass of the retroareolar region measuring 2.9 × 3.8 × 1.8 cm in size that was unchanged from previous imaging. Also noted was a new, slightly heterogeneous hypoechoic solid mass located 6 cm from the nipple at the 2 o’clock position measuring 2.7 × 1.2 × 2.4 cm. US guided biopsy of both masses revealed fibroadenoma.
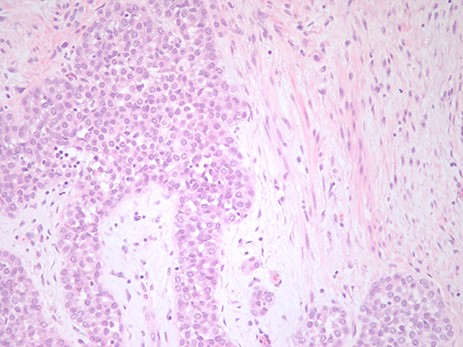
The pathological figure demonstrates LCIS in the background of a fibroadenoma. The image is at ×20 with an H&E stain.
Due to the painful and changing nature of the breast mass in the upper outer quadrant, she was offered left breast lumpectomy. In the operating room, a curvilinear incision was made over the palpable mass and dissection was carried down until the mass was encountered. Palpation was used to ensure that the entirety of the mass was excised. The cavity was also palpated with no residual mass left behind.
Final pathology demonstrated LCIS entirely confined to a large fibroadenoma (Fig 1). The mass measured 3.5 × 2.5 × 2.0 cm. There was no evidence of LCIS in the breast tissue surrounding the fibroadenoma.
Due to the pathology findings, she was taken to the operating room once more for excision of the remaining breast lesion. E-cadherin stain for LCIS within this mass was negative. An unremarkable fibroadenoma was the only finding.
DISCUSSION
In this case, a young female with a benign appearing breast mass was found to have a fibroadenoma containing LCIS. Although a rare finding, LCIS within a fibroadenoma may behave in a manner more consistent with a pre-cancer, rather than a general marker for risk. For this reason, she was taken for excision of an ipsilateral synchronous breast mass. This clinical scenario underscores the importance of examining specific imaging characteristics of fibroadenomas to determine risk for occult carcinoma within the lesion.
FUNDING
None.
CONSENT
The patient in this case provided informed consent.

{kind=link}