





Abstract
An anterior cruciate ligament (ACL) rupture is a common injury. The ACL usually tears in its mid-substance, an avulsion fracture of the ACL mostly occurs at the tibial attachment. In few cases, an avulsion fracture occurs proximally from the ACL attachment to the lateral femoral condyle. This is a rare finding, especially in elderly patients. We report a case of an avulsion fracture of the ACL attachment to the lateral femoral condyle after a traumatic injury in a 60-year-old female. Injury was not recognized during initial assessment, but was later detected during knee arthroscopy because of persisting mechanical complaints with catching of the knee. This emphasizes the importance of a thorough physical examination and magnetic resonance imaging. As rare as this condition is, it is important for the orthopaedic surgeon in treating these patients to include femoral end avulsion injuries of the ACL in the differential diagnosis.
INTRODUCTION
Anterior cruciate ligament (ACL) injury is common with an incidence of one in 3500 people, with sustained injury from non-contact sports and multi trauma as leading causes [1, 2].
Most injuries involving the ACL result in a tear of the ligament itself: mostly mid-substantially or at the attachment site of the lateral femoral condyle. However, a tear may also arise secondary to a bony avulsion fracture of the ACL. The most common avulsion site is the distal insertion to the tibia resulting in an (osteo)chondral avulsion fracture of the tibial spine [3, 4]. However, in rare cases, the ACL ruptures at the insertion site of the lateral femur condyle thereby creating an impaction fracture. This phenomenon can be difficult to recognize on a plain radiograph. In these cases, magnetic resonance imaging (MRI) can show a lateral femoral notch sign: a depression in the lateral femoral condyle, which could indicate an ACL tear [5]. This sign represents a severe bone contusion caused by impression, and microfracturing, visible on MRI, and is suspect for an impacted (osteo)chondral fracture due to a tear of the ACL.
We present a case of a 60-year-old female patient with an avulsion fracture of the ACL attachment to the lateral femur condyle. It is an uncommon injury especially in the elderly, and to our best knowledge we did not find a comparative report.
CASE REPORT
A 60-year-old female visited our outpatient clinic with a painful left knee and complaints of instability. She took a fall on this knee, 2 weeks earlier while hiking. Physical examination of the left knee showed intra-articular swelling along with limited range motion (flexion/extension: 30–5). A hematoma was seen superficial to the medial collateral ligament (MCL), which was painful on palpation. The ACL and menisci could not be assessed properly due to pain and swelling. Clinically, a grade 1 MCL lesion along with an ACL tear were suspected.
A conventional radiograph of the left knee showed no abnormalities (Fig. 1). An MRI scan was performed that confirmed an ACL tear accompanied by a grade 1 MCL tear, a lateral meniscal tear and a small incomplete fracture of the posteromedial tibia plateau (Fig. 2a–c). Arthroscopy of the knee was scheduled because of catching with persistent limited range of motion despite physical therapy 10 weeks after initial trauma.
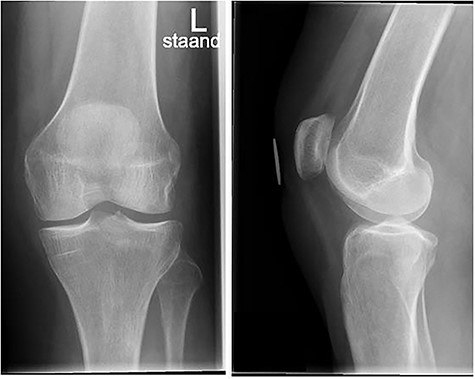
Conventional radiograph of the left knee shows no abnormalities.
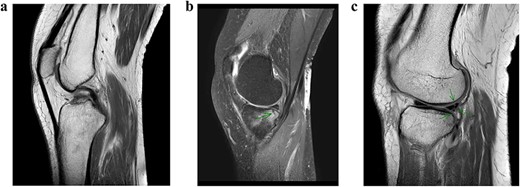
MRI scan of the left knee. (a) ACL rupture. (b) Small incomplete fracture of the posteromedial tibia plateau. (c) Partial lateral meniscal tear.
During arthroscopy, the ACL was torn proximally from the lateral femur condyle with an avulsion fragment. The lateral meniscus tear recognized on the MRI scan proved to be a double bucket handle lesion (Fig. 3). A partial lateral meniscectomy was performed and the insufficient ACL was debrided and removed along with the avulsion fragment.
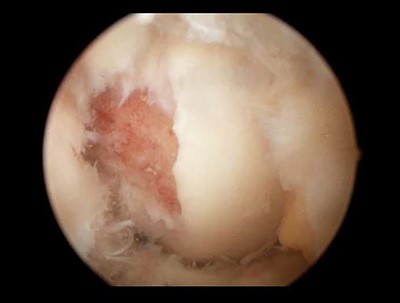
Knee arthroscopy showed an avulsion fracture from the ACL of the lateral femoral condyle.
Four weeks after surgery, the patient did not experience catching to any further extent and regained full function of her left knee (flexion/extension: 110–0). However, complaints about instability persisted. Physiotherapy was restarted for conservative treatment of an ACL tear.
DISCUSSION
As mentioned before, the most common tear site of the ACL is mid-substantially. When a tear of the attachment site involving a bony avulsion occurs, the distal tibia attachment is most likely involved. Avulsion fractures of the femoral ACL attachment are more rare: only 16 cases have been described of femoral ACL attachment bony avulsions. Thirteen cases were described in children, the remaining three in adults performing physical activity [6–8]. Avulsion fractures of the ACL typically occur in either strong external rotation of the tibia or internal rotation of the femur combined with a strong valgus load on the knee causing it to pivot shift [9]. In the immature skeleton, ACL avulsions are not uncommon due to relative weakness of the bone and greater elasticity of the connective tissue, and occur mostly at the distal tibial attachment site [10]. However, in the mature skeleton, a combination of bone maturation and deterioration of the ACL usually results in a mid-substance tear [10].
Nagaraj et al. [8] described a 20-year-old male athlete with a femoral avulsion of the ACL after a fall from a two-wheeler from resulting in a varus/endorotation injury of the knee. ACL reconstruction was performed using bone-patellar-tendon-bone-graft with good clinical results after 3 months.
Shah et al. [6] reported a 47-year-old female with an ACL femoral avulsion fracture accompanied by multiple fractures of the femoral and fibular shaft, tibia plateau as well as multiple ligamentous lesions. In this case, the avulsion could also have been a communitive fracture of the femoral shaft instead of an ACL-related injury. ORIF was performed and the avulsed fragment was fixated using screws.
Zabierek et al. [7] described a case of a 50-year-old male athlete with an ACL femoral attachment avulsion fracture after a pivoting knee injury during scuba diving, which was treated with fully threaded screws.
Several studies show (3D) CT imaging that can be useful in determining comminution, orientation, size and extend of the fracture as well as the integrity of the avulsed fragment [10]. These findings are of value in the course of treatment: either conservatively or surgically. However, patient-related factors and activity level are more important than the site of an ACL tear in (surgical) decision-making. In this case, the patient was a 60-year old non-athletic female. Therefore, we decided to debride the attachment of the ACL to the distal femoral condyle without a surgical reconstruction followed by physiotherapy to regain stability in daily life.
In conclusion, a bony ACL avulsion of the femoral condyle is rare, and diagnosis can be difficult. In the younger active patient with a large bony avulsion, treatment should be focused on anatomical reposition with preservation of the native ACL when possible, and otherwise ACL reconstruction to regain stability. To our knowledge, this is the first report of an avulsion fracture of the ACL attachment to the lateral femur in an elderly, non-athletic patient. Therefore, treatment was focused on regaining daily activity function.
Conflict of interest statement
None declared.
Funding
No financial support was received for this study.
Informed consent
Informed consent was obtained from the patient in this study.

{kind=link}
{kind=link}
{kind=link}