





Abstract
A case of bowel obstruction resulting from bael fruit (Aegle marmelos) in the rectum is described in an Indian Hindu elderly man. To our knowledge, this is probably the first reported case with such a presentation in available literature. Dilemma at unsuspecting clinical history and finding of clinical examination and imaging evaluation made the case more interesting and challenging to manage. The case also highlights the need for awareness, education about prevailing unregulated practice of traditional herbal medical therapy leading to disastrous consequences.
INTRODUCTION
Bowel obstruction is a very common surgical emergency. A number of causative factors have been identified that lead to mechanical bowel obstruction, and having foreign bodies in rectum is one of them. Retained foreign bodies in the rectum represent a common diagnostic and therapeutic challenge. The different modes and reasons for the insertion of foreign body in rectum have been described in literature, but history is more often misleading. Mostly, foreign bodies are inserted through anus intentionally; some are inserted by mistake but insertion for therapeutic purpose is rare. Most patients with rectal foreign bodies present to emergency department usually after efforts to remove at home are failed; thus, presentation is often delayed and complicated [1]. Bael fruit (Aegle marmelos) insertion in rectum as an herbal therapy that presented with bowel obstruction has never been reported in literature. We herein describe one such case in a 62-year old man and review the available literature.
CASE REPORT
A 62-year-old Indian Hindu man who was taking a traditional herbal medical therapy for his non-specific mild abdominal discomfort for an 8-year history, presented to the emergency department with a 6-day history of progressively worsening colicky abdominal pain, abdominal distension and constipation. He had no previous history of altered bowel habit, bleed per rectum or any urinary complain. He had never smoked, was non-alcoholic and had no other medical co-morbidity. On physical examination, he was mildly dehydrated, had distended, soft abdomen with no peritoneal signs and noted to have a palpable suprapubic bulge. On digital rectal examination, at 5 cm from the anal verge, we were surprised to feel a huge, hard, round tennis-ball-like mass, filling up whole of distal rectal lumen, making it difficult to insert a finger around the mass. The finger and thumb was put in to grasp and disimpact the mass back proximally, which then showed free movement in the rectum and had no pedicle. It felt smooth with some fine roughness over the surface and had a small opening on it. At that moment, we realised that a foreign body had been inserted through anus as a part of therapy; however, on further enquiry, the patient denied any such history.
The patient was further evaluated with flexible rectoscopy confirming the impacted mass, as endoscope failed to pass beyond it. Transabdominal ultrasonography, abdominal radiography and computed tomography (CT) scan of abdomen were obtained. CT scan demonstrated a large well-defined rounded peripherally hyperdense, internal hypodense object, likely a foreign body of size 5.7 × 5.6 cm noted in rectum causing focal distension of rectum with grossly dilated proximal bowel (Fig. 1a–d). Laboratory values were unremarkable. A differential diagnosis of foreign body or faecaloma in rectum leading to bowel obstruction was made.
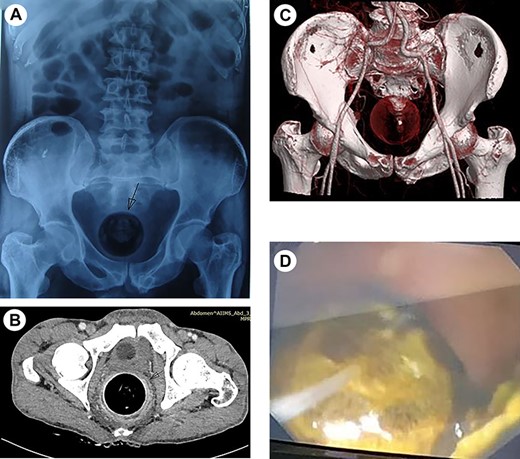
(a) Abdominal X-ray showing round foreign body in the rectum with dilated bowel loops. (b) CECT (axial) abdomen showing impacted foreign body in rectum and (c) the reconstruction image of foreign body in rectum. (d) Rectoscopic image showing rectal mass.
After resuscitating the patient, efforts to remove the mass per-rectally using manual, laxative, enemas, endoscopic means resulted in little success. The patient was taken to the operation theatre where he underwent manual evacuation under regional anaesthesia. The mass was successfully evacuated intact per-rectally, but after great difficulty (Fig. 2a–c). Enema and laxative were administered twice daily over next 2 days. The post-opearative recovery was uneventful.

(a) Operative image showing manual disimpaction and evacuation of foreign body through anus under regional anaesthesia. (b and c) Evacuated specimen of bael fruit and cut section showing vegetative material.
Histopathological examination of the specimen reported single, hard, swollen, brownish spherical mass of 50-mg weight. On cut section, cavity was identified filled with grey brown to black vegetative material that shown fungal hyphae under microscope. No atypia/malignancy was seen and no evidence of tissue invasion was seen.
On subsequent follow-up visit, it was told that a bael fruit had been inserted into rectum 4-year ago by a local practitioner of traditional medicine as a therapy. He also revealed that through an opening in the bael fruit, some more herbal preparation was added into, emphasising the religious belief. On further enquiry about the reason for putting it into rectum, he stated that the extract from bael fruit that he was receiving orally was not sufficient enough to relieve his abdominal ailments and he wanted long-term relief. He had denied these facts on initial visit out of fear and embarrassment. At a 6-month follow-up visit, patient was asymptomatic and doing well. Imaging evaluation was repeated and found unremarkable.
DISCUSSION
In some parts of India, particularly in rural and tribal population, the bael fruit extract has extensively been used as a traditional herbal therapy for various bowel ailments with proven efficacy [2, 3]. It is also noted that an age-old practice prevailing in these population to insert a bael fruit into vagina to prevent prolapse of the uterus presumably owing to its round shape, stringent action added with religious belief [4, 5]. Faecaloma and phytobezoar in rectum can also cause bowel obstruction [6, 7]. To remove these foreign bodies, several surgical and non-surgical methods are described. Our case was unique as a bael fruit was inserted 4 years ago as a part of therapy and history for insertion was misleading. The presentation was delayed until bowel obstructed. The successful evacuation of foreign body per-rectally with gentle manual disimpaction, under regional anaesthesia, could be a chance in our case that warrants a further study. Proper history taking and digital rectal examination are the cornerstones of reaching to diagnosis. Our case also highlights the urgent need for awareness and education, about such prevailing practices and there disastrous consequences with the aim to discourage and prevent patients getting into the trap of it.

{kind=link}
{kind=link}