





Abstract
An internal hernia is a protrusion of viscera through a congenital or acquired defect in the mesentery of peritoneum. They account for <0.9% of all small bowel obstructions [1] and ~4% of obstructions due to hernias [2]. We present a rare case of closed loop obstruction secondary to a band adhesion traversing the lower abdomen from a sigmoid colon appendage epiploicae to the right pelvic wall. A 82-year-old woman presented to the emergency department with nausea, vomiting and worsening right sided abdominal pain for 24 h, on the background of previous pelvic radiation and hysterectomy for uterine cancer. She was subsequently found to have a closed loop obstruction with 30 cm of ischemic bowel strangulated by a band adhesion from a sigmoid colon appendage epiploicae to the right abdominal wall. The patient underwent a successful small bowel resection with primary anastomosis and made an uneventful recovery.
INTRODUCTION
An internal hernia is a protrusion of viscera through a defect in the mesentery of peritoneum, the defects can be congenital and/or acquired. Congenital internal hernias include paraduodenal, pericaecal, Foramen of Winslow, transmesenteric and transmesocolic hernias while acquired internal hernias can occur after pelvic or bowel resectional surgery, Roux-en-Y gastric bypass, trauma and/or secondary to inflammation [1]. They account for <0.9% of all small bowel obstructions (SBO) [1] and ~4% of obstructions due to hernias [2]. We present a case in which a sigmoid colon epiploic appendage adhesion to the right pelvic wall resulted in a closed loop obstruction.
CASE REPORT
A 82-year-old woman presented to Emergency Department (ED) with 24 hours of nausea, vomiting and worsening right sided abdominal pain. Patient reported that her bowels were last open 2 days ago and has since been unable to pass any flatus with increasing abdominal bloating. Her medical history included well controlled type 2 diabetes mellitus, hypercholesterolemia and hypertension. Her surgical history was significant for a hysterectomy 25 years prior for uterine cancer for which she also received pelvic radiation. Her blood tests on presentation revealed a white cell count of 8.46 109/L and a C-reactive protein of 3 mg/L with haemoglobin, platelets, electrolytes and liver enzymes all being within normal limits, as were her vitals.
An abdominal examination revealed a focal tenderness over her right lower quadrant and right pelvis and generalised abdominal distention. Computed tomography (CT) scan (Fig. 1a and b) showed small bowel faecalisation in the distal small bowel with a focal bowel loop in the right iliac fossa displaying engorgement of its mesentery with moderate volume of free fluid in the right paracolic gutter and Morison’s pouch. Findings were highly suspicious for a closed loop bowel obstruction with bowel wall compromise.
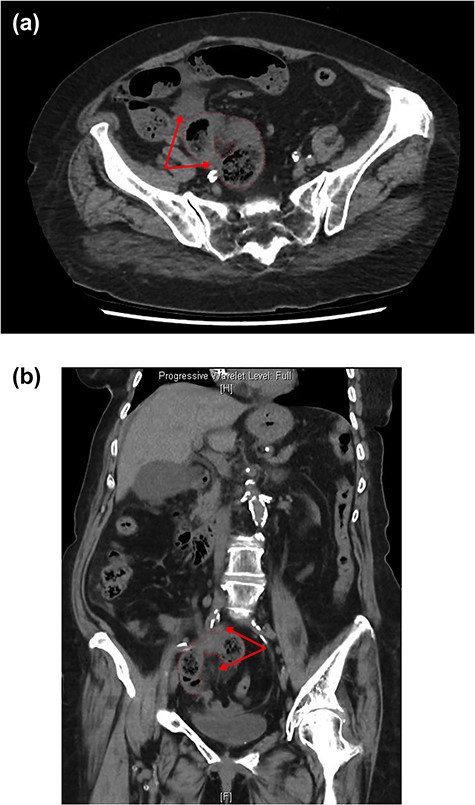
CT axial (a) and coronal (b) views showing loop of strangulated small bowel with surrounding fat stranding and free fluid (red arrows).
The patient was taken to theatre for an exploratory laparotomy where the proximal jejunum was dilated and serous fluid in the peritoneal cavity was noted. There was herniation of 30 cm of jejunum through a defect created by a tight band adhesion traversing the lower abdomen between an appendage epiploicae on the lower sigmoid colon and its attachment to the right pelvic wall (Fig. 2a and b). The strangulated loop of small bowel was ischemic and necrotic at the time of operation with no macroscopic evidence of perforation. The band was released and the bowel was run and no other areas of compromise were noted. The patient underwent segmental jejunal resection with a side to side double layered hand sewn anastomosis and made an uneventful post-operative recovery. Histology confirmed ischemic enteritis in the resected small bowel segment with adjacent acute serositis without evidence of perforation.
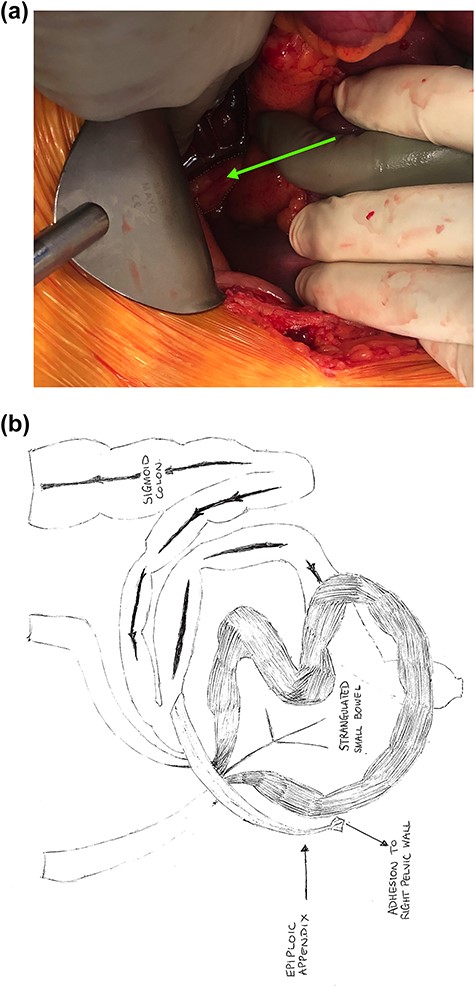
(a) Intraoperative image demonstrating loop of strangulated small bowel (red border) and band adhesion to the right pelvic wall (green border and arrow); and (b) schematic depiction of the closed loop obstruction.
We deduce that a combination of pelvic radiation and subsequent hysterectomy had contributed to the formation of the adhesive band.
DISCUSSION
Acquired internal hernias are, although rare, an important cause of SBO, and its diagnosis and appropriate treatment may be challenging. A history of chronic intermittent attacks of vague abdominal cramps with previous abdominal surgery may be suggestive of the diagnosis. CT imaging has high diagnostic accuracy in both detecting SBO and defining its severity and aetiology [3, 4]. Due to the increased risk of bowel entrapment with acute strangulation and bowel infarction, even a small internal hernia is dangerous.
Our case highlights the importance of early surgical intervention as internal hernias can present with non-specific abdominal symptoms and normal bloodwork. We advise surgeons to be observant of CT imaging and consider prompt operative intervention where required.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}