





Abstract
Glomus tumor (GT) is a rare, benign neoplasm of the glomus apparatus. Being most common in the subungual region, it often misdiagnosed with dermatological conditions. Severe tenderness, paroxysmal pain and cold intolerance symptomatically denote GT. Clinical tests such as Love’s pin test and Hildreth’s test assist in diagnosing the disease. X-ray, ultrasonography and magnetic resonance imaging can confirm the severity of the lesion. Complete surgical excision is the only treatment available for these subcutaneous nodules. A middle-aged male with a hand pain, who misdiagnosed for dermatitis over 15-year period, has identified as having a large bone-boring GT. Awareness of GT among healthcare professionals is a must to increase the quality of life of patients.
INTRODUCTION
A glomus tumor (GT) is a rare tumor of the glomus apparatus situated in the reticular dermis. They are often benign, though few incidences reported of malignancy [1, 2]. They occur commonly in the subungual region of the fingers, though evidences support for widespread throughout the body [1–3]. GTs are rare, accounting for 1–5% of the soft-tissue tumors of the hand [4–6]. As of their rare incidence and misleading clinical presentation, GTs are often misdiagnosed with other diseases.
GT is characterized by severe tenderness on palpation, paroxysmal pain and cold intolerance. Love’s pin test, Hildreth’s test and cold-sensitivity test are commonly used to identify GTs [6, 8]. X-rays, ultrasonography and magnetic resonance imaging (MRI) scans are essential in confirming the diagnosis [7]. The only efficient treatment for GT is complete surgical removal.
Being a disease that has cloaked for ages, GT should be paid much attention in early diagnosis and recovery. This case presentation describes a large bone-boring GT that was mistakenly treated as a chronic dermatological condition for 15 years.
CASE REPORT
A 52-year-old male presented to the Outpatients’ Hand Clinic with a history of significant pain, skin changes and itchiness in the right little finger for 15 years. He was referred from the dermatology clinic for a skin biopsy, suspecting either dermatitis, Lichen Simplex or viral warts. Over the past 15 years, the patient was seen by numerous specialists as of failure in proper diagnosis.
At the clinic, the patient was examined thoroughly. He was suffering from a constant deep throbbing pain (9/10 numeric pain scale) throughout the day and night. He required non-steroidal anti inflammatory drugs (NSAIDs) and opiates regularly to alleviate the pain. Yet, the itching of the ulnar aspect of the hand and little finger was not relieved with medication. The patient described paroxysmal pain on dishwashing, especially with cold water. Clinical examination showed exquisite pressure tenderness over the tip of the right little finger with positive Love’s pin test and Hildreth’s test. The signs, symptoms and clinical tests supposed the condition to be a GT. X-rays, ultrasound scan and contrast-enhanced MRI confirmed the lesion of 16 × 8 × 7mm to be a GT (Figs 1 and 2).

Little finger MSK ultrasound—19 July 2018 ‘16 × 8 × 7 mm’ soft tissue lesion involving the nail bed and wrapping around the terminal phalanx of the right little finger suspicious for a GT.
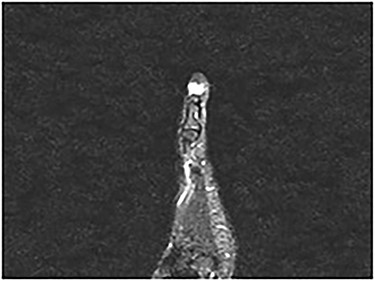
Right hand MRI—19 August 2018 ‘8 × 9 × 10 mm’ hyperintense lesion resulting in pressure erosion and bone remodeling of the distal phalanx keeping with subungual GT.
A large, bone-boring GT was found to penetrate through distal phalanx, reaching the volar aspect of the pulp. Surgical excision of the tumor was performed under local anesthesia using a hockey-stick incision.
Complete pain relief was noted immediately after the surgery. Follow-up after 1 year did not reveal any evidence of recurrence.
DISCUSSION
Glomus apparatus in situ in reticular dermis facilitates thermoregulation. These neuromyoarterial bodies regulate the peripheral blood flow by operating as an arteriovenous anastomosis specifically designed to control body temperature and blood pressure. Rarely, this glomus apparatus proliferates into a neoplasm which disturbs its functionality. Glomus bodies locate throughout the body. Thus, GTs can arise in various segments of the body including forearm [1], arm [3], sternum [3], calf [3] and GI Tract [2], other than the subungual region.
Symptoms of GT include the classic triad, severe tenderness, paroxysmal pain and cold intolerance. It may also present with swelling at the nail plate [5, 6], nail irregularity [7] and subcutaneous/nail discoloration [4, 6] (Fig. 3). GTs can often get misdiagnosed as inflammatory or musculoskeletal conditions due to swollen, painful nodules [7].

Image demonstrating subcutaneous discoloration and skin changes of the little finger found in our patient.
Three tests are commonly utilized to distinguish GT in the clinical setting: Love’s pin test, Hildreth’s test and cold-sensitivity test [6, 8, 9]. Positive Love’s pin test exhibits a decline in classic severe pain when the nail/skin overlying the nodule gets pressed with a sharp object such as a pinhead [9]. The Hildreth’s test was considered to be positive, if the characteristic pain and tenderness alleviates by inflating the tourniquet applied to the upper limb and worsens by deflating it [8, 9]. Positive cold-sensitivity test indicates severe paroxysmal pain when submerging the affected area in cold water [9].
The exact location of the tumor is to determine by imaging studies. While plain radiographs being the primary imaging technique [4, 5], contrast-enhanced MRI (commonly T2-weighted images) clearly shows the nodule and its margins [5–7]. Ultrasonography is effective in detecting GTs, regardless of the challenges such as nail curvatures which may disturb the continuity of the reporting and small, even tumors which may difficult to distinguish [6].
In our case, the patients’ chronic skin changes due to the constant itchiness lead to several incorrect diagnoses by the dermatological team such as dermatitis, lichen simplex and viral warts (Fig. 3). The patient had nail discoloration mimicking subungual hemorrhage and dystrophic nail changes that can be seen in dermatitis [10]. The patient has also undergone an MRI, 8 years ago, for a suspected cervical nerve root compression as of the pain and itching of ulnar aspect of hand. This misleading performance of the condition delayed the referral to the plastic surgical team. On his referral to the plastic surgical team, a high suspicion for GT immediately established after the physical examination, in which he showed the typical triad of GT clearly. He has undergone a right-hand X-ray, an ultrasound and an MRI to confirm the diagnosis.
Surgical removal of the tumor can perform under a tourniquet technique [3, 4, 7, 8] or general anesthesia [7]. Literature supports surgical approaches such as trans-ungual [4, 5, 6, 7], lateral subperiosteal [4, 6], Keyser–Littler [6] and volar [4, 6] approach for the GTs in fingers. Our patient underwent a surgical excision using a hockey-stick incision under local anesthesia, which has hardly found in the literature for this purpose. After the surgery, he showed excellent recovery with the cessation of his symptoms within 1 year.
Complications of the surgery, including infection of the surgical site, nail bed deformities and recurrence [8], can be prevented by complete, reiterative wide excision [4].
Subungual GTs often get misdiagnosed for other medical conditions. This case has demonstrated a lack of knowledge regarding this disease among healthcare professionals. This patient had a poor quality of life due to his symptoms for 15 years, which could have been easily avoided if he has referred promptly. It is important to raise awareness of this medical condition to promote early referral and improve care for this patient group.
CONFLICT OF INTEREST STATEMENT
None.

{kind=link}
{kind=link}
{kind=link}