





Abstract
The aim of this study is to illustrate the managements of different clinical and radiological presentations of serious complications of frontal sinusitis diagnosed and managed at the tertiary referral hospital. A case series study conducted at the tertiary referral in the period from 2012 to 2019. Four different cases of serious complications of frontal sinusitis namely orbital abscess, frontal meningitis, subdural empyema and frontal lobe abscess will be presented and discussed. Despite the generous use of antibiotics, the serious complications of frontal sinusitis still develop. The serious complications of frontal sinusitis ranges from orbital abscess to frank frontal lobe abscess. The management is a combination of systemic antibiotics and surgical drainage with excellent outcomes.
INTRODUCTION
Rhinosinusitis is defined as inflammation of the mucosa of the nasal cavity and the paranasal sinuses, detected by either clinical, endoscopic or radiological findings. According to its duration rhinosinusitis is considered acute if it lasts for >12 weeks, and chronic if <12 weeks. Frontal sinusitis is a relatively common condition that affects 15% of the adult population. It presents as frontal headache, fever, tiredness and may be accompanied by tenderness over the medial part of the infraorbital margin. The frontal sinuses are asymmetrical paired structures that are separated by the intersinus septum. Due to its close relation to many vital structures, frontal rhinosinusitis may lead to various dangerous complications, which may be fatal [1].
The orbital complications of the frontal sinusitis may progress to become as severe as to cause total loss of vision on the affected eye. The causative mechanism of this complication is due to the anatomical relationship from the frontal sinus to the orbit, in which the floor of the frontal sinus is directly superior to the orbit. The extension of infection could be by direct invasion or by retrograde thrombophlebitis [1]. These complications include preseptal cellulitis, orbital cellulitis, subperiosteal abscess, orbital abscess, the latter of which may lead to blindness [2]. Further extension to the middle cranial fossae may lead to intracranial complications, such as meningitis, epidural empyema, subdural abscess, brain abscess and cavernous sinus thrombosis [2].
The diagnosis of the frontal sinusitis’ complications is based mainly on the clinical evaluation in addition to other diagnostic modalities, such as anterior rhinoscopy, x-rays and computed tomography (CT) scans which are considered the standard test of choice for the evaluation of complicated rhinosinusitis. However, magnetic resonance imaging (MRI) is more sensitive in the evaluation of orbital and intracranial involvement [3, 4].
After making the diagnosis of these complications, prompt treatment is needed which usually requires multidisciplinary teams because patients may progressively deteriorate and lead to death [2]. Fortunately, morbidity and mortality of these complications are decreasing substantially since the introduction of new generations of antibiotics, endoscopic sinus surgeries and neuronavigation [4].
The aim of this study is to illustrate the managements of different clinical and radiological presentations of different serious complications of frontal sinusitis diagnosed and managed at a tertiary referral hospital.
METHODS
This is an 8-year case series study, from January 2012 to November 2019. It was conducted in the ENT department in Saudi Arabia.
RESULTS
Five different cases of serious complications of frontal sinusitis namely orbital abscess, frontal meningitis, subdural empyema (SDE), frontal lobe abscess and frontal osteomyelitis with frontocutaneous fistula will be presented and discussed.
Illustrative Cases
Case 1: orbital abscess
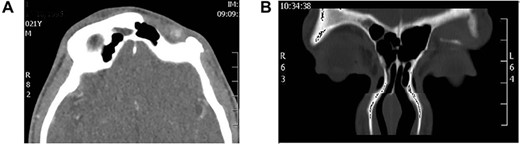
A 12-year-old girl referred from the pediatrics hospital as a case of complicated sinusitis presenting with fever, progressive infected left eye, restricted eye movement and diminished vision (Fig. 1A). CT scan sinuses and orbit (Fig. 1B) showed a severely inflamed frontoethmoid sinuses associated with extensive frank orbital abscess. The patient was managed with intravenous antibiotics and underwent urgent endoscopic frontoethmoidictomy and endoscopic drainage of orbital abscess. Patient recovered fully with no complications (Fig. 1C).
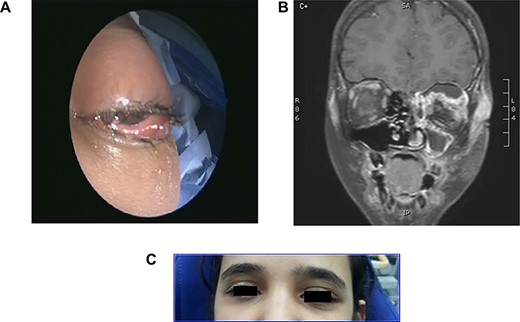
(A) Severly infected left eye with restricted movement, (B) CT sinuses and orbit with inflamed frontoethmoid sinuses and orbital abscess and (C) 6 weeks post-treatment.
Case 2: meningitis with superior sagittal sinus thrombosis
Young girl with 2-week history of unresolving sinusitis presented with fever, headache, vomiting and drowsiness diagnosed as a case of bacterial meningitis as a complication of frontal sinusitis. MRI (Fig. 2A) showed a left frontal sinusitis, meningitis and sagittal sinus thrombosis. Patient underwent endoscopic drainage of the sinuses with a combination of intravenous antibiotics. Patient had an excellent recovery with no complications, as shown in post-treatment MRI (Fig. 2B).
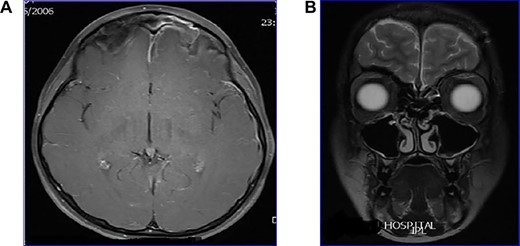
(A) MRI showing frontal sinusitis with meningitis and sagittal sinus thrombosis, (B) post-treatment MRI with clean sinuses and brain.
Case 3: subdural empyema
Young girl presented with unresolving sinusitis associated with fever, headache, vomiting and drowsiness. Diagnosed on CT brain as a case of SDE (Fig. 3A and B) as a complication of frontal sinusitis. The patient was managed by systemic intravenous antibiotic. Endoscopic frontal sinusotomy and frontal mini craniotomy to drain the empyema by the neurosurgery team. The patient recovered well with no complications as shown in follow-up CT scan (Figure 3C).
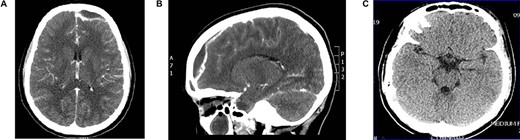
(A) axial CT brain with subdural empyema, (B) sagittal CT scan with subdural empyema and (C) post drainage CT brain with complete resolution of subdural empyema.
Case 4: frontal lobe abscess
Young man referred as a case of frontal lobe abscess as a complication of untreated frontal sinusitis. The patient presented with fever, headache and changes in personality and mood. Coronal MRI brain (Fig. 4A) showed a large frontal lobe abscess and an inflamed frontal sinusitis as in Fig. 4B. the patient was managed with a combination of intravenous antibiotics, endoscopic frontal drainage and frontal craniotomy to drain the frontal abscess by the neurosurgery team. Patient tolerated the procedures well with no complications as shown in postoperative CT brain (Fig. 4C).
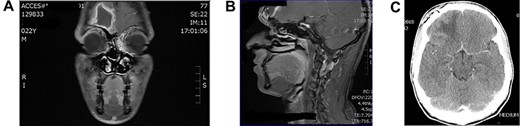
(A) Preoperation coronal MRI brain with large frontal lobe abscess, (B) preoperation sagittal MRI of frontal lobe abscess extending from inflamed frontal sinus and (C) post drainage CT brain showing complete resolution of the frontal abscess.
Case 5: frontal bone osteomyelitis with frontocutaneous fistula
Young man complaining of chronic left frontal pain with discharging fistula above his left eyebrow. CT scan showed an inflamed frontal bone secondary to his frontal sinusitis (Fig. 5A). Coronal CT sinuses (Fig. 5B) confirmed the diagnosis of frontal osteomyelitis and discharging frontocutaneous fistula. The patient underwent endoscopic sinusotomy with external debridement of infected frontal bone with closure of fistula. Patient improved with no evidence of recurrence.
(A) Axial CT scan showing left frontal bone osteomyelitis and (B) CT sinuses showing left frontal bone osteomyelitis with discharging fistula.
DISCUSSION
Endoscopic sinus surgery (ESS) is now the standard procedure in treating complicated cases of frontal sinusitis. It was suggested after the development of the endoscopes and made it possible to avoid unnecessary open surgical techniques. As the variability of the extends and the complications of the frontal sinusitis. Therefore, many classifications have been suggested but the most accepted classification is that described by Draf in 1991 [1]. A thorough anatomical understanding in addition to good skills and experience is the key to successful surgeries with fewer complications. To reach better results, it is required to do the essential preoperative assessment involving taking the appropriate imaging scans.
Endoscopic management of the intraorbital complications of frontal sinusitis has been shown to be effective [3], however, the role of ESS is not clear yet in managing intracranial complications. Furthermore, since most of the intracranial complications are not resulting from direct extension of the infection, it is not surprising that surgical drainage of the sinus does not appear to achieve immediate results. In contrast, ESS in conjunction with antibiotic administration is indicated if the intracranial complications appear to be resulting from a direct extension. Drainage of the intracranial purulence while pursuing the definitive surgical management for the affected sinus using ESS is considered to be the popular intervention, especially for SDE [4].
Orbital complications of frontal sinusitis are varied. Orbital abscess is one of the most serious complications. It is known as the purulent inflammatory pus collection in the retro-orbital adipose tissue. This complication was found in three cases out of 35 of orbital complications in one healthcare center from 1999 to 2009. The process often starts with inflammatory edema. Then, the upper eyelid may show some changes due to fluid accumulations that are caused by the restriction of the venous return. In this phase, the vision usually is not affected, and the eyeball movement is intact. If untreated, this will progress and becomes more severe when proptosis is noticeable, which indicates the shifting of the infection toward cellulitis. The condition will be more severe to a degree that may weaken the vision, and the eyeball movements will be restricted due to the compression on the optic nerve. If the condition persists without any treatment it may shift to an orbital abscess, in which purulent inflammation develops. The symptoms vary and may include, other than that mentioned, exophthalmos, ophthalmoplegia and loss of vision can sometimes occur. This form could lead to more complications as septic thrombosis of the cavernous sinus or intracranial spread through nerve routes [3]. In this case, surgical intervention is the only option as the medical conservative treatment will not be as rapid. A case reported by Altman et al. of a 13-year-old male with orbital abscess was managed by external decompression of the orbital abscess in addition to maintaining sufficient drainage of the frontal sinusitis [6].
Frontal sinusitis could also give rise to another set of complications which is intracranial complications. It is less common than orbital complications, but it can cause severe morbidities [6]. These complications may include frontal lobe abscess which is defined as the collection of purulent inflammatory pus within the brain frontal lobe [6]. The route of spread could be direct by structural defects, or by hematogenous spread. The clinical manifestations are not specific and may include mild fevers vomiting headaches, personality changes and/or mood swings. Advanced frontal lobe abscesses may cause epileptic attacks [6]. These complications mostly require neurosurgical intervention.
Osteomyelitis, as a complication of frontal sinusitis, usually occurs due to either direct extension of the infection to the frontal bone, or through thrombophlebitis of the diploic veins. It usually affects children and adolescents and considered to be rare in adults. Osteomyelitis due to other paranasal sinusitis is rare. Osteomyelitis can lead to the development of subperiosteal abscess of the frontal bone, which is called Pott’s Puffy Tumor (PPT), and if perforated it leads to the formation of a frontocutaneous fistula. Epidural and subdural abscess as well as meningitis can result alongside PPT [2, 7]. Patients with PTT present with tender forehead swelling with pitting edema [7]. In most cases, systemic antibiotics along with subcutaneous or ESS are sufficient in treating this condition. A craniotomy can be necessary in case of intracranial involvement. Recent literature has shown that performing intranasal ESS along with simple percutaneous drainage is effective in treating this condition [7]. A case reported by Tatsumi.et al. about a 46-year-old man who presented with PPT and was initially managed with incisional drainage. Subsequently, the patient was referred to the rhino-otolaryngology department and underwent successful ESS. He had no recurrences of PTT thereafter [7]. Another case reported by Chokkalingam et al. about a 72-year-old woman who presented with frontal osteomyelitis due to frontal rhinosinusitis and forehead swelling, which was initially managed with incisional drainage. Four months later the patient presented to the otolaryngology department with forehead fistula. Subsequently, the patient has undergone transfistula endoscopic closure of the frontocutaneous fistula [8].
Meningitis occurs most commonly as a result of extra-axial suppurations from intracranially complicated frontal sinusitis. In most of the studies, epidural and subdural abscesses are found to be the usual intracranial complications, whereas others suggested that meningitis is the more common. Szyfter et al. reported that 80% of meningitis cases occurred in association with other intracranial complications [9]. The most common complications resulting from meningitis include seizures and hearing loss [5]. Management of meningitis includes administration of intravenous antibiotics and fluids, and if there is no response for 24–48 hours, surgical intervention is needed [2]. ESS is considered as the main surgical option. Younis et al. reported seven cases of sinusitis associated meningitis, all of which were managed with systemic antibiotics and ESS [10].
SDE was considered the most common intracranial complication of frontal rhinosinusitis; however, recent studies suggest that epidural abscess is more common. These intracranial complications occur as a result of the spread of infection from the frontal sinus to the anterior cranial fossa, which then turns to abscess formation [7]. Patients with SDE are usually febrile, present with meningism and signs of systemic infection [2]. On imaging, SDE usually appears as hypodense crescent-shaped, rim enhanced collections that cross the sutures but not the midline, and usually detected using CT scans [7]. The mortality rate of SDE ranges from 10% to 70%, hence it is considered as a neurosurgical emergency [4].
Substantial morbidity can be exhibited by patients who have a history of SDE, which includes hemiparesis in 15–35% of cases, seizures in 12–37.5% of the cases and residual neurologic deficits in almost half of the cases. SDE is usually managed surgically in conjunction with antibiotic therapy [4]. DelGaudio et al. reported six cases of SDE that were initially managed with ESS and intravenous antibiotics. Five of the six cases eventually underwent craniotomy due to the nonresponsive rapidly progressive condition [5].
CONCLUSION
Despite the generous use of antibiotics, the serious complications of frontal sinusitis still develop. The serious complications of frontal sinusitis range from orbital abscess to frank frontal lobe abscess. The management consists of a combination of systemic antibiotics and surgical drainage with excellent outcomes.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}