





Abstract
Mucocele of the appendix refers to an appendix that is distended by mucus and transformed in a mucus-filled sac. Appendicular torsion is rare. Primary and secondary forms of appendicular torsion are known. Our patient presented to the emergency department with complaints mimicking acute appendicitis. Imaging with computed tomography and ultrasound showed a cystic lesion most likely originating from the right ovary. The veriform appendix was located close to this lesion and seemed to be distended. During diagnostic laparoscopy, a torsion of the veriform appendix due to a mucocele was found and an appendectomy was performed. Histopathological analysis confirmed the diagnosis. Torsion of the vermiform appendix is most often diagnosed intra-operatively. Pre-operative radiologic imaging is often not useful in the detection of appendicular abnormalities other than acute appendicitis. The treatment consists of detorsion and appendectomy.
INTRODUCTION
A mucocele of the appendix refers to an appendix that is distended by mucus and transformed in a mucus-filled sac [1, 2]. The term mucocele was first used in 1842 by Karl Freiherr von Rokitansky and an appendicular torsion was first described in 1918 [1, 3]. Appendicular torsion is rare and patients present themselves often with complaints mimicking acute appendicitis. In a recent overview of literature, 33 cases of appendicular torsion were described [4]. Primary and secondary forms of appendicular torsion are known. Primary torsion is associated with an anatomical variation of the appendix [3, 5]. Secondary torsion is often the result of an appendicular abnormality, such as a mucinous cystadenoma or a simple mucocele [3]. We present a case of torsion of the vermiform appendix due to a mucocele.
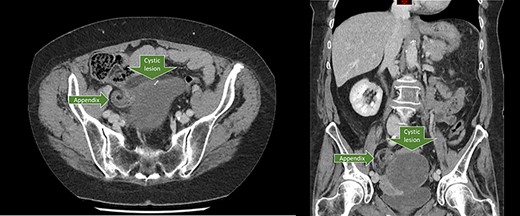
Axial and coronal CT-scan showing the dilated appendix in close proximity to the cystic lesion.
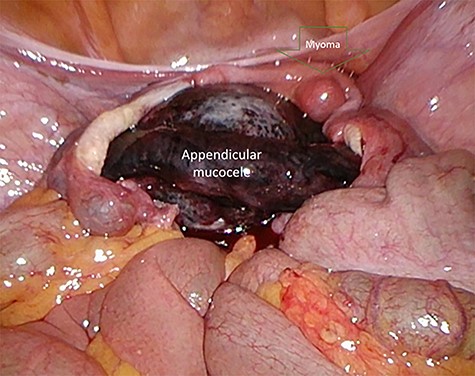
Pre-operative image of a small uterus myoma and the appendicular tumor with ischemic discoloration due to the torsion.
CASE Report
A 66-year old female patient, with a past medical history of hypertension, presented to the emergency department with a central stomach ache radiating to the upper and lower abdomen. Complaints initiated that morning and were continuously present in varying severity. The pain was accompanied by nausea, vomiting and anorexia. The patient had normal vital parameters with a pulse rate of 82 beats per minute and a temperature of 37.4°C. Physical examination of the abdomen showed tenderness in the suprapubic region. Laboratory results were normal except a leukocytosis of 11.2 x 10*9/L [reference 4–10 x 10*9/L]. Urinalysis showed positivity of nitrate, and presence of some leukocytes and erythrocytes. The presumptive diagnosis was an urinary tract infection for which an urine culture was performed, and antibiotics were prescribed. Because of the atypical presentation, the patient was reassessed at the emergency department the following morning. The complaints were persistent and the abdominal examination still showed tenderness in the suprapubic region but at this moment also in the right lower quadrant (RLQ). Laboratory results showed a C-reactive protein (CRP) of 57 mg/L (reference 0–5 mg/L) and a leukocytosis of 13.2 x 10*9/L. A computed tomography was performed and showed a large cystic lesion with wall calcifications in the RLQ measuring 8.6 x 7.1 x 9.6 cm probably originating from the right ovary (Fig. 1). The appendix was situated in close proximity to this abnormality, and measures 6 mm at the base and 1.1 cm more distally, with infiltration of the surrounding intra-abdominal fat. The appendix looked rotated to caudal. One of the differential diagnosis was a torsion of the right ovarium. An additional ultrasound was carried out by the radiologist to try to clarify the anatomical origin of the abnormalities, but was inconclusive. Informed consent was obtained for a diagnostic laparoscopy with a gynecologist standby. During laparoscopy, inspection of the intra-abdominal genitals showed no abnormalities besides a small myoma of the uterus. The appendix showed a large tumor, which was twisted several times at its base and was purple/ischemic discolored (Fig. 2). After complete detorsion, the appendix was stapled with an endostapler and the appendix was retrieved through a Pfannenstiel incision. The patient recovered without any complications and was discharged home the next day. Histopathologic investigation showed a cystic cavity with a calcificated wall filled with mucus and confirmed the diagnosis of low-grade mucinous neoplasm of the appendix, with reactive changes due to the torsion. There were no signs of perforation and the appendix was removed completely. The patient was discharged from follow up after 8 days.
DISCUSSION
Torsion of the vermiform appendix is a rare disorder that presents with clinical signs similar to acute appendicitis. It is therefore often diagnosed intra-operatively. Primary torsion of the appendix can be the result of a long appendix and a fan-shaped mesoappendix with a narrow base or the absence of azygotic folds which attach the appendix laterally [3, 4, 5, 6]. Secondary torsion might be caused by the presence of abnormalities such as a fecalith, lipoma or appendicular mucocele [2, 4]. The latter is divided into non-neoplastic variants (mucosal hyperplasia and mucosal retention cyst) and neoplastic variants (mucosal adenoma, low-grade mucinous neoplasm and mucinous cystadenocarcinoma) [2].
Although the appendicular torsion is most often diagnosed intra-operatively, some findings on pre-operative radiologic imaging could suggest the presence of a torsion, particularly secondary torsions. For instance, an appendicular diameter of more than 15 mm is suggestive for a mucocele with a sensitivity of 83% and a specificity of 92% [2]. Also the presence of wall calcifications is suggestive for a mucocele [2]. A missed diagnosis pre-operatively is however not catastrophic, because the differential diagnosis often includes acute appendicitis or torsion of one of the ovaries and also require a diagnostic laparoscopy. Treatment of the appendicular torsion is dependent on the cause. In case of a primary torsion without any abnormal lesions, an appendectomy is sufficient [3]. Also in the case of a mucosal hyperplasia, mucosal retention cyst, mucosal adenoma and low-grade mucinous neoplasm limited to the appendix, an appendectomy is required [7]. One should always be aware to avoid rupture of the appendicular mucocele, because the spread of mucinous content throughout the abdominal cavity can provoke pseudomyxoma peritonei [4]. This condition has a poor 10 year survival rate of 10–30% [1]. In case of mucinous cystadenocarcinoma, a right hemicolectomy is required with lymphadenectomy [7]. In practice, the diagnosis is often definitive after histopathology and in case of a mucinous cystadenocarcinoma of second operation is necessary after simple appendectomy.
Concluding, torsion of the vermiform appendix can present with symptoms similar to acute appendicitis. It is most often diagnosed intra-operatively. Pre-operative radiologic imaging is often not useful in the detection of appendicular abnormalities other than acute appendicitis. The treatment consists of detorsion and appendectomy. It is important to minimize the risk of rupture in case of a mucocele to avoid the spread of mucinous content to the abdominal cavity. In case of a malignant lesion, an additional right hemicolectomy with lymphadenectomy has to be performed. In primary torsions or secondary torsions, due to a benign abnormality, an appendectomy is sufficient.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
INFORMED CONSENT
A written informed consent was obtained from the patient.

{kind=link}
{kind=link}