





Abstract
This is a rare case of a 42-year-old Hispanic male with macrodactyly who presented with recurrent carpal tunnel syndrome (CTS) due to Lipofibromatous Hamartoma (LFH). A slowly growing mass in his right palm with pain and numbness, along with motor and sensory deficits in the median nerve distribution, was reported since the past year prior to visit. Previous open carpal tunnel release was performed at 16 years of age due to CTS without complications. The diagnosis of LFH was made based on ultrasound, electromyography test and physical examination. An extended open carpal tunnel release with transection of transverse ligament was performed. The 24-month postoperative evaluation showed complete resolution of symptoms. This report illustrates the management of a recurrent CTS due to LFH in a Hispanic adult patient with macrodactyly that was successfully treated with a carpal tunnel decompression.
INTRODUCTION
Lipofibromatous Hamartoma (LFH) is a rare isolated peripheral nerve tumor that commonly affects the median nerve during childhood [1]. This benign fibroadipose tumor affects the median nerve at the carpal tunnel segment in 80% of cases [1]. The exact origin of this condition is unknown; and one-third of cases present with macrodactyly [2]. Most LFHs are treated at an early age with decompression of the median nerve at the wrist due to carpal tunnel syndrome (CTS) [2].
Limited reports have established the recurrence of CTS in children with LFH, with no reports among patients with macrodactyly [3–5]. This article illustrates the first case of recurrent CTS due to LFH in a Hispanic adult patient with macrodactyly that was successfully treated with a carpal tunnel decompression.
CASE REPORT
A 42-year-old Hispanic male presented to our orthopedic clinics with a 1-year complaint of progressive pain, numbness, tingling and swelling, in the thumb, index and long finger of his right hand and distal forearm. Initially, the patient felt frequent nighttime awakenings, difficulty eating and significant limitation at his warehouse job. A painless mass between the palm and wrist, which was observed since childhood, started to gradually increase in size since the onset of symptoms. No trauma or family history was reported. Further history revealed an uncomplicated open carpal tunnel release (CTR) due to CTS at 16-years of age; with complete resolution of initial symptoms until recurrence of symptoms, 1 year prior to our visit.
Physical examination showed macrodactyly with ulnar deviation of second and third digits of right hand along with palmar wrist scarring from previous surgery. A localized, single, palpable 4 × 2-cm tender subcutaneous mass was appreciated over the right volar wrist and distal forearm. Muscle weakness was apparent in the thenar intrinsic, abductor pollicis brevis, opponens pollicis and flexor pollicis brevis muscles, without hypoesthesia. Radial pulse and capillary refill were normal. Tinel’s sign and Phalen’s test were both positive without evidence of thenar muscle atrophy (Fig. 1).

Clinical photographs of a Hispanic adult with macrodactyly and Lipofibromatous Hamartoma (red arrow).
A high frequency ultrasound showed a 5.4-cm × 1.3-cm × 2.8-cm ventral hypoechoic fusiform shape mass in continuity with the median nerve; going from the flexor tendon and muscles, to the carpal tunnel distally. Electromyography test confirmed decreased conduction velocity and motor latency prolongation of right median nerve along with median entrapment neuropathy at the wrist. Radiographs showed middle finger soft tissue swelling with calcified phlebolith without erosive changes.
Surgical exploration with decompression of the median nerve was performed under regional block anesthesia and a longitudinal incision extending from the distal forearm to the midpalm. Right thick transverse carpal tunnel ligament sheath under a tan color mass was seen arising from median nerve. Removal of scar tissue and extended release of transverse ligament was performed without complications (Fig. 2). An uneventful postoperative recovery was shown with no neurological deficit. The 24-month postoperative evaluation showed complete resolution of pain, numbness and tingling; with healed surgical wounds and no signs of infection.
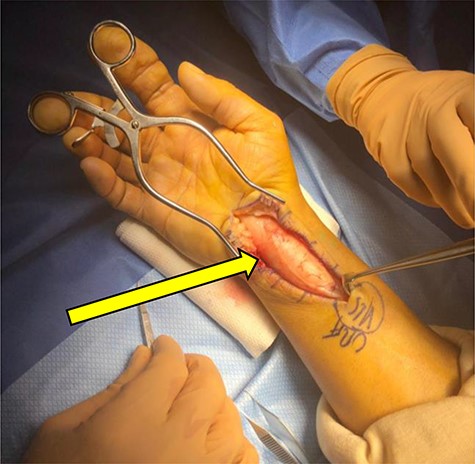
Intraoperative photographs of a Hispanic adult with lipofibromatous hamartoma (yellow arrow).
DISCUSSION
The LFH is a rare benign peripheral tumor that infiltrates nerves by fibroadipose tissue, causing an enlargement to median nerve at carpal tunnel segment in 80% of cases [6]. Previous reports have shown that LFH presents before 30-years of age in 71% of cases [7]. Macrodactyly has been associated with LFH in 30% of cases [1]. Although the etiology of LFH is unknown; congenital mass presentation, history of trauma to median nerve and previous surgery have been proposed as risk factors related to its development [2]. In our case, the patient had a previous CTS surgery during adolescence with no history of trauma.
To date, the influence of ethnicity in LFH is unknown despite its description in multiple cases [5, 6, 8]. Silverman and Enzinger described the ethnic distribution of LFH in 14 white patients and 1 black patient [5]. Additionally, two other case reports presented LFH in Caucasians [6, 8]. We believe that ethnicity should be evaluated as a possible risk factor of LFH in future studies.
Clinical diagnosis of LFH is challenging since there are no physical findings that are pathognomonic for distinguishing it from other conditions [2]. Differential diagnosis of LFH includes neurofibroma, ganglion cyst, among others [2, 7]. A fundamental aspect for LFH management is the distinction from nonencapsulated nerve tumors such as neurofibromas; which are difficult to differentiate visually. However, the lack of neurocutaneous manifestations and family history in our patient allowed the differentiation of LFH from neurofibromatosis [7].
The use of either ultrasound or magnetic resonance image (MRI) is used to diagnose LFH without the need of biopsy [9]. The ultrasound at affected area usually appears with an enlarged, thick fascicle in a fusiform shape surrounded by echogenic fatty tissue [9]. By contrast, MRI tends to illustrate an enlarged nerve with thick axonal bundles surrounded by an epineural fibrous tissue [9]. Even though radiographs cannot give an imaging diagnosis for LFH, they are recommended in patients with macrodactyly to evaluate hypertrophic bone changes and possible expansion of soft tissue [2].
Due to its rarity, there are no guidelines regarding LFH treatment in symptomatic patients with recurrent CTS. A variety of surgical options ranging from the release of carpal tunnel to the complete median nerve excision have been described [8]. Nowadays, complete nerve excision is rarely recommended due to possible fibrofatty tissue infiltration within nerve bundles, and risk of permanent neurologic deficit [10]. Current treatment options are now focused on a conservative approach toward the relief of patient symptoms. A common approach is the open CTR by excision of transverse carpal ligament, which has shown adequate results with pain relief and improvement in the strength of the opponens pollicis muscle [7, 8].
Among the general population, reoperation for CTS has been reported in up to 12% of cases, mainly due to incomplete transection of transverse carpal ligament [10]. Despite the lack of observational studies, previous reports have described recurrence of CTS in children with LFH, without associated macrodactyly [3–5]. We present the first case of a recurrent CTS in a Hispanic adult with macrodactyly and LFH of the median nerve.
Surgical decompression was proven as treatment alternative in patients with LFH, showing excellent results with no sensory or motor deficit. Clinicians should consider LFH in their differential diagnosis in Hispanic patients with macrodactyly who present with slow-growing masses and compression neuropathy.

{kind=link}
{kind=link}