





Abstract
The prevalence of transmesocolic hernias, a subtype of internal hernias (IHs), is generally low. Its clinical consequences, including strangulation, ischemia and even death, however, necessitate awareness. IHs are classified as congenital or acquired as resulting from surgery, trauma or intraperitoneal inflammation. This is a case of a 37-year-old male victim of a motor vehicle collision 1 month prior to the index admission. The trauma-related injuries were managed conservatively and then discharged home. The patient was re-admitted with a 2-day history of epigastric pain, vomiting and abdominal distension. A diagnosis of small bowel obstruction due to a transmesocolic hernia was made on CT and emergency laparotomy performed. The post-operative course was unremarkable. It is vital to consider transmesocolic hernias in trauma patients presenting with a picture of bowel obstruction even in the absence of prior surgery.
INTRODUCTION
Internal hernia (IH) is a protrusion of intra-abdominal viscera through an anatomical or abnormal opening of the peritoneal cavity, leading to strangulation or incarceration [1, 2]. IH are rare causes of acute abdomen and small bowel obstruction in 0.6–5.8% of the cases [3]. Although the recorded autopsy incidence is 0.2–0.9%, if strangulated and left untreated, IH has an overall mortality rate of more than 50% [4]. There are several locations where IH can be localized, with paraduodenal (53%) being the most common and transmesenteric consisting of transmesocolic (8%) and transomental (1–4%) being the rarest [2]. IHs can be congenital or acquired, where congenital transmesenteric hernias are more common in children and are extremely rare in adults. The previous surgery, trauma history or peritoneal infection are the most common risk factors for acquired internal transmesocolic hernias in adults [1, 2].
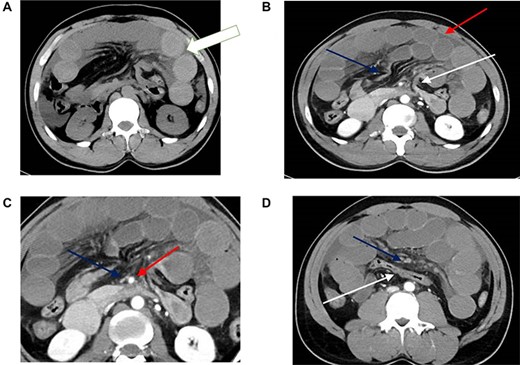
CT scan findings of transmesocolic hernia. (A) CT scan demonstrates hyperdense appearance of small bowel loops (arrow) suggestive of intramural hemorrhage. (B) Contrast enhanced CT scan demonstrates internal hernia with dilated bowel loops (red arrow), afferent loop at dudenojejunal junction (white arrow) and efferent loop (blue arrow). There is associated mesenteric congestion and free fluid. (C) Marked attenuation of the superior mesenteric vein (blue arrow) compared to the adjacent superior mesenteric artery (red arrow). Note also the congestion and fan-like. (D) The transverse colon (white arrow) is seen posteriorly with the congested small bowel mesentry (blue arrow) and dilated small bowel loops seen anterior to it. Note also the poor enhancement of the mesenteric veins.
IH may be clinically asymptomatic or may cause distress ranging from persistent vague epigastric pain to intermittent colicky periumbilical pain, whereas nausea and vomiting are additional symptoms [5, 7]. The diagnosis of an IH by physical examination is difficult and the most effective diagnostic form is abdominal computed tomography (CT) especially the observation of peripherally located small bowel, and lack of omental fat between the loops and the anterior abdominal wall [6, 7]. In addition, clustering of small bowel loops and an abnormality in the mesenteric vessels are also useful observations on abdominal CT.
In patients having IH, timely surgical intervention based on clinical suspicion and/or CT scanning findings is advisable for its management [4]. Due to the high morbidity and mortality rates, it is required to reduce the strangulated intestinal segment as early as possible to avoid intestinal ischemia, necrosis and perforation and thereby minimize resection levels [8]. The laparoscopic technique has been found effective for the diagnosis and treatment of intestinal obstruction. In rare cases, trauma can also lead to transmesocolic hernias with no previous surgical history. In this case report, we have reported a case of transmesocolic hernia due to recent trauma without a history of surgery.
CASE REPORT
A 37-year-old male presented with a 2-day history of severe epigastric pain, non-radiating, and associated with nausea and postprandial vomiting at the Trauma center on 11 March 2020. The patient also reported two episodes of hematemesis in the emergency department that day. Reports passing stool and flatus normally; furthermore, he did not report melena or per rectal bleeding. He refuted any history of the same pattern of symptoms before.
The patient had a pertinent history of involvement in a motor vehicle collision about a month before the presentation. It was a head-on collision at high speed; the patient was not wearing a seatbelt. He sustained a traumatic injury to the third part of the duodenum and the inferior surface of the pancreas. He was managed conservatively and discharged. He did not have a relevant past medical history and he is a heavy smoker.
On general examination, the patient was a middle-aged man, in apparent abdominal discomfort. He was tachypneic (25 breaths/min) and tachycardic (118 beats/min). Blood pressure reading was 114/78 mmHg. Systemic examination of the abdomen revealed a distended abdomen. The distension was symmetrical and moving with respiration. Palpation revealed tenderness and guarding in the epigastric region. On percussion, dullness was detected around the epigastric region, while hyperactive bowel sounds were heard on auscultation. A digital rectal examination was conducted and revealed normal tone, no masses, no blood and stool in the vault.
Laboratory examination showed leukocytosis of 14 000/mm3 with normal lactate (0.8 mmol/l). An erect abdominal X-ray, including the diaphragm, did not show evidence of free peritoneal fluid. Abdominal CT (Fig. 1) showed dilatation of small bowel loops with a focal area of narrowing at the duodenal jejunal flexure and ileum, with the apparent collapse of small bowel and colon distal to the ileal narrowing. Furthermore, the posterior displacement of the colon was revealed. CT also revealed an abrupt narrowing of the superior mesenteric vein with poor opacification of the distal branches.
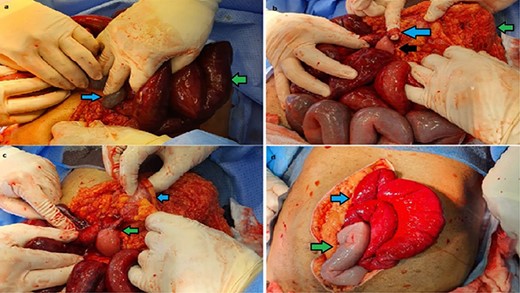
Intra-operative findings of transmesocolic hernia. (A) blue arrow: mesenteric defect with small bowel; green arrow: congested, near ischemic bowel. (B) green arrow: transverse colon; blue arrow: adhesive band; black arrow: small bowel protruding through transverse colon mesenteric defect. (C) blue arrow: transverse colon; green arrow: retrieved small bowel herniated through the mesenteric defect. (D) post closure of defect; green arrow: small bowel regaining normal color; blue arrow: hyperemic small bowel.
A tentative diagnosis of small bowel obstruction was made, and emergency laparotomy was performed. Intra-operatively (Fig. 2), a herniation of the small bowel through the transverse mesentery was noted. The hernia contained all of the small bowels which had dusky discolored loops. Adhesions between the mesentery and small bowel loops were also noted. There was however no bowel perforation or frank gangrene; in addition, no injury or ischemia to the transverse colon was noted. The small bowel was reduced and rewarmed, followed by the closure of the defect on the transverse mesentery. No bowel was resected. The small bowel maintained its dusky discoloration even after rewarming; the superior mesenteric artery, however, regained normal physiologic pulsations. The post-operative course was uneventful.
DISCUSSION
An IH is the outpouching of viscera through the peritoneal coverings or mesentery. This could result from congenital defects or acquired through surgery, trauma or intraperitoneal inflammation. IHs are named according to the location per the welch classification. In order of commonality, these are paraduodenal hernias (53%), pericecal (13%), transmesenteric (8%), hernias through the foramen of Winslow (8%), supravesical and pelvic (6%), intersigmoid (6%) and finally transomental (1–4%) [9]. The clinical presentation of IH can be asymptomatic or symptomatic. In symptomatic patients, the presentation is that of recurrent colicky abdominal pain, dyspepsia and vomiting. IHs run a risk of strangulation and ischemia, which can be life-threatening. This risk is particularly profound in transmesocolic hernias, which account for up to 40% of all IHs strangulation [10]. The diagnosis of IH is dependent on CT imaging. However, in our case, it was diagnosed intra-operatively as the CT scan finding immediately post-trauma did not show IH. Diagnostic findings include indicators of a closed-loop obstruction that include a U- or C-shaped, distended loop of intestine that is also fluid-filled. The convergence of radiation of distended loops with thickened mesenteric vessels is the other sign. Swift open emergency laparotomy is the mainstay management option.
CONCLUSION
Even though rare, transmesocolic hernias should be suspected in patients presenting with a picture of small bowel obstruction or an acute abdomen post-trauma even in patients without prior surgeries.
AUTHORS’ CONTRIBUTIONS
DS, MA, AA, AZ and ME—study concept, data collection, surgical therapy for the patient.
DS, MA, AA, AZ and ME—surgical therapy for the patient.
DA, MA, RS and ME—writing original draft.
AZ, HA, ME, RS and AE—review and editing draft.
CONFLICTS OF INTEREST STATEMENT
None declared.
FUNDING
None.
ETHICAL APPROVAL
This case report was approved by medical research center at HMC (MRC-04-20-405).
CONSENT
No identifiable images of the patient were used for the publication of this case report.

{kind=link}
{kind=link}