





Abstract
Pectus excavatum is a chest wall deformity with an incidence of around 1 in 400 live births. The Nuss procedure is a surgical intervention that aims to restore functional integrity in these patients. We report the first case of bar migration into the stomach necessitating further surgical intervention for removal. Our case presents a rare complication of pectus excavatum repair and highlights the importance of vigilant follow-up in these patients. If bar migration does occur, imaging in the form of X-ray and CT scans may be of use in early detection in order to expedite management.
INTRODUCTION
Pectus excavatum (PE) is a chest wall deformity with an incidence of around 1 in 400 live births [1]. The deformity affects the anterior chest wall and is caused by abnormal growth of the sternum and adjacent ribs producing a concave appearance of the chest. Patients with pectus excavatum often complain of dyspnoea, fatigue and exercise intolerance. In severe cases, cardiac compression is reported. Surgical correction is one option for these patients and minimally invasive surgical techniques are becoming the most favourable option. The Nuss procedure aims to restore functional integrity by the insertion of one or two stainless steel bars behind the sternum. These bars will lift the deformity and be stabilized for a period of 2–3 years before their removal [2].
CASE REPORT
We report the first case of bar migration into the stomach necessitating further surgical intervention for removal.
A 22-year-old male patient with pectus excavatum was evaluated in our thoracic surgery clinic with a view to undergo surgical correction in the form of the Nuss procedure. His clinical history and general practitioner report revealed that he had been suffering with dyspnoea for the last 3 years. His preoperative lung function tests showed decreased maximal expiratory flow at 50% and vital flow capacity of 25%. The preoperative computerised tomography (CT) scan showed a Haller index of 5.7.
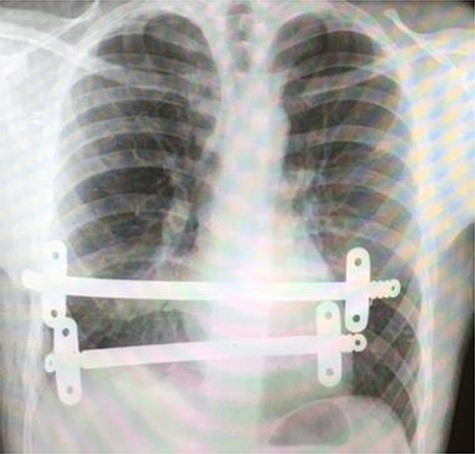
Postoperative chest X-ray following initial Nuss procedure, showing both substernal bars inserted to elevate the depression caused by pectus excavatum.
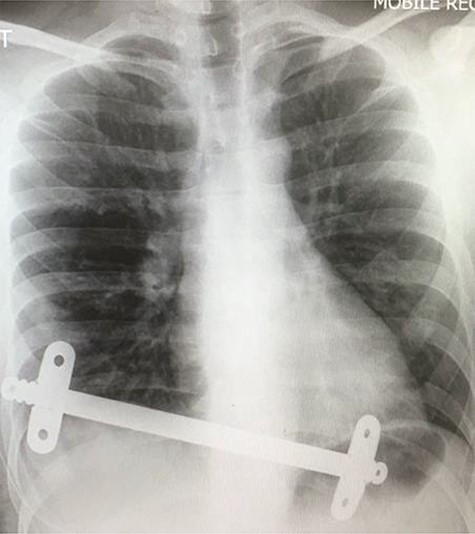
Chest X-ray taken after the removal of the upper substernal bar. The second bar is seen, traversing the diaphragm, having migrated into the stomach.
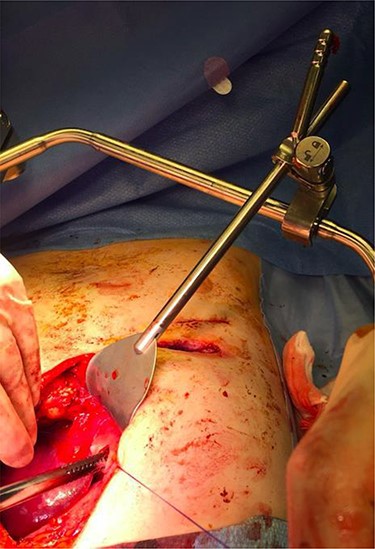
Superior lateral intraoperative view of the laparotomy used to access and remove the second migrated bar.
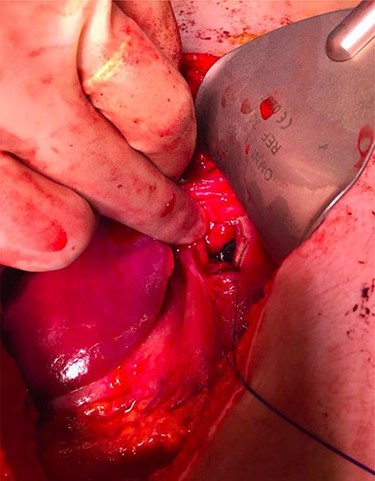
Superior intraoperative view of the laparotomy used to access and remove the second migrated bar.
The patient underwent video-assisted thoracoscopic surgery (VATS) and the modified Nuss- procedure for the surgical correction of his PE. The primary incision was 0.5 cm long along the anterior axillary line of the right lateral chest in the second intercostal space. A 5-mm zero-degree thoracoscope was used to provide clear visualization. An additional 2-cm incision was made, 10 cm underneath the previous incision, where the bar introducer and an 11-inch bar were inserted for correction of the PE. This bar was secured using one stabilizer on each side. An additional second 9-inch Nuss bar was inserted inferior to previous bar with one stabilizer on each side. The procedure was uneventful, and a chest X-ray was performed to confirm adequate substernal bar placement (Fig. 1).
Our patient was followed up annually. After two and half years, he developed a right-sided wound infection, initially treated with antibiotics. It was decided to remove the bar for prevention of recurrent infection. The chest X-ray showed migration of the lower-placed bar (Fig. 2). The upper bar and associated stabilizers were removed through the bilateral small incisions without any complication; however, the lower bar was not palpable. Therefore, a left-side thoracotomy was performed; however, the bar was not found in the chest. The incision was extended to a midline laparotomy (Fig. 3). This revealed an erosion of the bar in to the stomach after passing over the left lobe of the liver (Fig. 4). The bar and stabilizers were completely removed, and the hole in the stomach was closed directly with sutures. The patient was discharged home without any further complication after successful recovery.
COMMENT
The Nuss procedure is a well-established surgical procedure that aims to restore physiological function and alleviate symptoms in patients with PE. Complications have been reported based on lack of experience and technical insufficiency [3]. Pneumothorax is often the most common complication. Whilst bar displacement has been reported previously in literature, it is still rare and usually confined to the thoracic cavity [3]. Although stabilizers reduce the rate of bar displacement, this complication remains a significant problem in the context of the Nuss procedure [4], and several other techniques have been proposed in order to try and reduce the risk of bar dislodgement. The use of steel wires to fix the Nuss bar to the adjacent rib reliably secures the bar and minimizes bar migration [5].
We report this case as it is a rare complication of pectus excavatum repair but highlights the importance of vigilant follow-up in these patients. If pectus migration does occur, then X-ray and CT may all be beneficial in early detection and the management of such a complication.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}