





Abstract
Gouty arthritis commonly occurs in peripheral synovial joints and involvement in the thoracic cage is extremely rare. We report a case of a 52-year-old presenting with a painful bony mass in her sternal notch. Imaging demonstrated a lobulated calcified and necrotic lesion causing mass effect on adjacent structures. Excision biopsy confirmed a benign cystic lesion with amorphous material containing needle-shaped refractile crystals suggestive of uric acid. Tophaceous gout was diagnosed. Presence of a periarticular mass with characteristics of gout should warrant investigation with biopsy and imaging. This can prevent misdiagnosis of malignancy and avoid unnecessary surgery in asymptomatic lesions.
INTRODUCTION
The sternoclavicular joint (SCJ) is a diarthrodial saddle joint. It is formed by the sternal end of the clavicle, the clavicular notch of the manubrium and the cartilage of the first rib [1].
Common causes of SCJ swellings include trauma, infection and arthritis (rheumatoid, septic and degenerative). It is also important to rule out malignancy (primary and secondary causes) in patients who present with SCJ swellings. We report a rare case of increasing bony swelling in the sternal notch and left SCJ due to tophaceous gout.
CASE REPORT
A 52-year-old fitness instructor, who was previously fit and well, presented with a painful bony mass in her sternal notch, which had increased in size over 3 years. She reported issues with swallowing and change in voice that worsened with forward flexion of the head.
Both magnetic resonance imaging (MRI) and computed tomography (CT) scanning demonstrated a lobulated calcified and necrotic mass of 3.9 cm by 4.3 cm on the left SCJ causing a mass effect on adjacent structures (Fig. 1). Anteriorly the mass was bordered by the sternocleidomastoid muscle and dorsally by the sternohyoid muscle. There was compression of the left hemi-thyroid causing displacement of the trachea. There was no direct contact with the aorta or brachiocephalic vein.
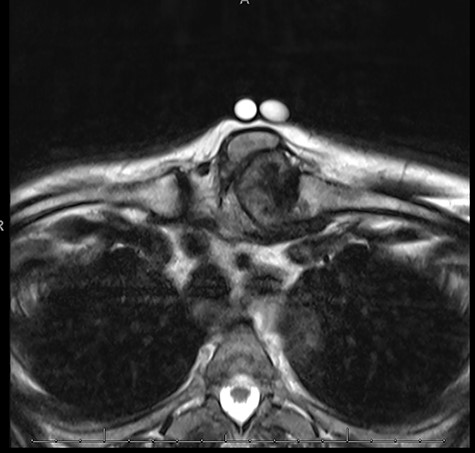
MRI sternoclavicular joint showing lobulated calcified and necrotic mass of 3.9 cm by 4.3 cm on the left SCJ causing a mass effect on adjacent structures; anteriorly the mass is bordered by the sternocleidomastoid muscle and dorsally by the sternohyoid muscle.
Differentials included synovial osteochondromatotis and malignancy. Biopsies of the lesion were non-diagnostic and therefore excision biopsy was carried out for diagnosis as well as symptomatic improvement.
Using a trans-cervical incision, the tumour was superficially shelled-out sparing the sternocleidomastoid on the right and partially preserving the left sternocleidomastoid insertion on the left. With a combination of sharp and blunt dissection, the tumour was dissected away from deep tissues and shaved off the manubrium and excised. The left clavicle head was then removed separately. The bony tumour with a casseous quality appeared to arise from the left clavicular head and did not involve the deeper vascular structures. The excised tumour was sent to histopathology.
Expert review was sought from the Royal National Orthopaedic Hospital, and the specimen was confirmed to be a benign cystic lesion with amorphous deposition. Under polarized light, the amorphous material contained needle-shaped refractile crystals suggestive of uric acid. Therefore, a diagnosis of tophaceous gout was made.
DISCUSSION
Gout is the manifestation of systemic disease. It often stems from high levels of uric acid in the blood, leading to the formation and deposition of monosodium urate crystals in tissues. When the crystals surround the joint, this results in tophi. The worldwide prevalence of gout is around 1–4% of the general population and is increasing due to poor dietary habits, lack of exercise and obesity [2].
The first metatarsophalangeal joint is most commonly affected in gout. Other common sites include the midtarsal joints, ankles, knees, fingers, wrists and elbows. Tophaceous gout located in the SCJ is an extremely unusual condition. From our literature search, we have found evidence of only two cases of true gout affecting the SCJ prior to this case [3, 4].
Common investigations to consider in patients with suspected gout include full blood count, renal function, lipids, glucose, thyroid function and serum urate concentration (although this may be low during an acute attack). The best diagnostic test is aspiration of fluid from an affected joint for the identification of urate crystals [5]. Although in practice, this rarely occurs as many patients are diagnosed based on clinical findings. In fact, based on the Health Professionals Study only 11% of patients with gout had diagnostic aspirations [6].
In our case, the unexpected location in which the bony swelling occurred led to a lower index of suspicion of gout. Fedeli et al. [4] describe the use of duel-energy CT (DECT) to help diagnose gout in cases of doubt or unusual locations. With this technique, it is possible to differentiate uric acid crystals within the bone from calcium-based dystrophic calcification.
Based on a single centre study of 40 patients, the sensitivity and specificity of DECT for diagnosing gout were 0.90 and 0.83, respectively [7].
Although on this occasion, initial biopsies were not diagnostic, the presence of a periarticular mass with the characteristics of gout (despite being in an unfamiliar location) should warrant investigation with biopsy and further imagining. This may help to prevent the misdiagnosis of malignancy and avoid unnecessary surgery in asymptomatic lesions.
Disclosures
The authors have nothing to disclose.

{kind=link}