





Abstract
Adenomyomas are benign tumours made of smooth muscle cells, endometrial glands and stroma. An extrauterine location is extremely rare with an unknown pathogenesis. Preoperative diagnosis is challenging and pathologic examination is necessary to confirm the diagnosis. Here we present a case report of a 44-year-old woman with a painful non-reducible mass in the right inguinal region without fever or other alarming symptoms 2 months after a laparoscopic hysterectomy. She was treated with a surgical resection of the mass. Extrauterine adenomyoma is a very uncommon entity. Preoperative workup is challenging, as confirmation of the diagnosis can only be achieved by histopathological analysis following surgical excision.
INTRODUCTION
Adenomyomas in extrauterine sites are an extreme rare entity [1]. It encompasses a benign tumour composed of endometrial glands and stroma, surrounded by thick-walled smooth muscles [2]. The most common site of extrauterine adenomyoma is the ovaries. The pathogenesis of extrauterine adenomyomas is still unclear. However, there is some evidence of hormonal influences, embryologic developmental errors and mechanical/iatrogenic mechanisms leading to these tumorous abnormalities [3, 4]. A preoperative diagnosis is challenging to establish. Surgical excision provides a definitive diagnosis after histopathological examination and is mostly curative in case of benign pathology [1, 2]. This case report presents a rare case of a painful extrauterine adenomyoma arising in the inguinal region in a 44-year-old woman.
CASE REPORT
A 44-year-old multiparous woman (gravida 2, para 2), with a gynaecologic medical history of two caesarean sections at the age of 26 and 31, presented with a painful non-reducible mass in the right inguinal region without fever or other alarming symptoms. Two months prior to presentation a total laparoscopic hysterectomy was performed (without a salpingo-oophorectomy) because of menometrorrhagia. The intact uterus was removed vaginally and there were no complications in the postoperative phase. Histopathological analysis of the uterus was consistent with the preoperative diagnosis of adenomyosis. Additionally, two leiomyomas were found, one subserosal and one intramural, with a maximum diameter of 0.8 cm. Clinical examination revealed a palpable non-reducible regular mass of 3.0 ×2.0 cm in the right inguinal region near the round ligament of the uterus. Inguinal ultrasonography (US) showed a 2.2×1.4 cm hypoechoic solid mass suspicious for malignancy (Fig. 1). Because of the initial suspicion for malignancy, diagnostic workup also included an ultrasound of the abdomen and a chest X-ray, which showed no abnormalities. Laboratory investigations including white blood cell count, kidney and liver function were within normal ranges. Serology for Bartonella henselae antibodies was negative excluding cat-scratch disease. An ultrasound-guided biopsy was performed to obtain histology. Microscopic examination of the biopsy showed a leiomyomatous lesion, without signs of malignancy. The surgeon performed a resection of the mass. During the procedure, the mass was located proximal of the inguinal ligament and fixated in the inguinal ring. The mass was removed without any complications. Inspection of the specimen revealed a 1.8 × 1.8 × 1.5 cm white–gray regular mass surrounded by yellow–gray tissue. The histologic findings were consistent with extrauterine adenomyoma (Fig. 2). The patient was discharged within 24 h after surgery. The patient remained asymptomatic without any signs of recurrent disease after 1.5 years of follow-up.
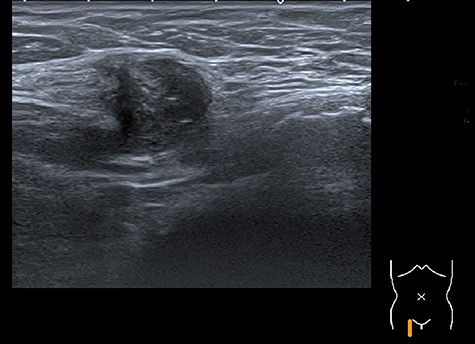
Image of the inguinal ultrasound that shows an inhomogeneous round mass surrounded by subcutaneous fat tissue.
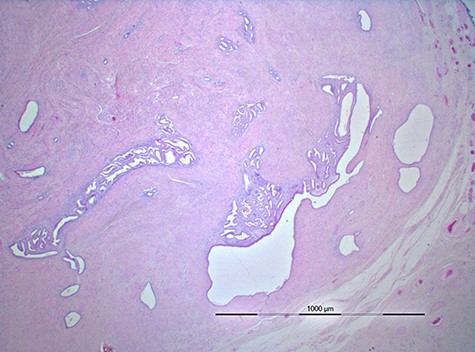
Image of histopathology shows a well-circumscribed lesion composed of foci of benign endometrial glands and endometrial stroma surrounded fat and connective tissue.
DISCUSSION
Extrauterine adenomyoma is a very uncommon entity. A few cases have been described in the current literature. Most of these cases were pelvic adenomyomas located in the pararectal space, ovaries and broad ligament [1]. However, extrapelvic located adenomyomas are also reported, for instance in the caecum, descending colon and mesocolon [2]. Cases of extrauterine adenomyomas located in the upper abdomen are also known [5].
The pathogenesis of extrauterine proliferation of adenomyomatous tissue is not fully understood yet because of its rarity. However, various theories suggest that the development of extrauterine adenomyomas is multifactorial. Rosai et al. [6] proposed the theory of a defective Mullerian duct fusion to explain the extrauterine location of adenomyomas. In a few cases, this theory is supported by the fact that adenomyomas are associated with congenital anomalies in these patients, such as renal agenesis, double excretory system and anomalies of the lower genital tract [7]. Cozzuto et al. obtained for a theory of smooth muscle cell metaplasia. This theory suggested that an already existing focus of endometriosis undergoes metaplasia into smooth muscle, explaining the pathogenesis of adenomyoma [3]. Redman et al. established the sub-coelomic mesenchymal metaplasia theory. This specific layer lies below the mesothelial surface of the peritoneum and contains multipotent cells that have the capacity to differentiate and proliferate into the endometrial stroma, smooth muscles and even decidua under hormonal stimulation [4]. Batt et al. proposed the last theory of embryological origin: the theory of Mullerianosis. It states that a heterotropic organoid structure of embryonic origin composed of Mullerian cell rests may get incorporated into normal organs at the time of organogenesis. This theory provides an explanation for unusual extrapelvic locations of adenomyomas [8]. Another widely reported mechanism is the spread of cells during (morcellated) hysterectomy or myomectomy [9].
The most common presenting symptom of extrauterine adenomyomas is abdominal pain, often associated with menstruation-related symptoms such as intermenstrual spotting, menorrhagia, dysmenorrhea or metromenorrhagia [1, 2]. A history of gynaecologic surgery might be relevant, such as a hysterectomy or myomectomy [1]. However, no conclusive predisposing risk factors have been described regarding the development of extrauterine adenomyomas.
A preoperative diagnosis of extrauterine adenomyoma is challenging because of the rarity and therefore lack of structured guidelines. A recently published review of the literature showed that in 34 cases no certain diagnosis was made preoperatively, even with the usage of different preoperative imaging modalities, such as US, computed tomography and magnetic resonance imaging. Our patient only received a US [1]. The tumours seen on these imaging methods are often falsely mistaken for a malignancy. However, histopathologic examination is always required and the gold standard for definitive diagnosis.
The histopathology is that of a well-circumscribed lesion composed of foci of benign endometrial glands and endometrial stroma surrounded by hyperlastic smooth muscle bundles. In this case, the lesion was located in and surrounded by fat and connective tissue.
Surgical excision is the first choice of treatment for extrauterine adenomyomas [1]. Our patient also received a surgical treatment without complications or medical treatment afterwards. In addition, there are some authors who obtain for a medical treatment of monthly GnRH agonists after surgery to stop the estrogen-stimulated proliferation of the neoplastic tissue to prevent recurrence [10].
This is an interesting and rare case of a woman with an extrauterine adenomyoma, located in the inguinal region 2 months after a laparoscopic hysterectomy. Preoperative workup is challenging, as confirmation of the diagnosis can only be achieved by histopathological analysis following surgical excision. Therefore, surgery remains the first choice of treatment.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}