





Abstract
Shiitake mushroom is a common ingredient in East Asian cuisines. Food processing/preparation can cause the mushroom to be soft and slimy, leading to accidental swallowing. Due to its high insoluble fibre content, it remains the same size and shape in the intestinal tract. We present two cases of small bowel obstruction caused by shiitake mushroom requiring surgical intervention. Preoperative imaging showed dilated small bowel with a suspicious mass in the ileum. However, the exact cause was unclear. For both cases, exploratory laparotomy and enterotomy were then performed and undigested shiitake mushroom was found. Both patients recovered well from the surgery.
INTRODUCTION
Small bowel obstruction is most commonly caused by adhesions due to previous abdominal surgery or hernias. Other causes include strictures, intussusceptions, tumours and gallstone ileus. Rarely, small bowel obstruction can be caused by bezoars, with reported frequencies of ~4% [1]. The word bezoar is derived from the Arabic word ‘bazahr’, which means the hardened stomach contents of Syrian goats [2]. There are four types of bezoars, depending on the constituting material of the indigestible mass such as phytobezoars (vegetables and fruits), trichobezoars (hairball), pharmacobezoars (medications) and lactobezoars (milk). Here we present two cases of small bowel obstruction caused by the same causative agent, shiitake mushroom, that occurred during the first week of Chinese New Year in Malaysia.
FIRST CASE
An 86-year-old Chinese gentleman presented with 1 day history of vomiting and colicky abdominal pain. He had underlying hypertension and cerebrovascular accident >10 years ago. On examination, his abdomen was distended but soft. There was mild tenderness at paraumbilical region. However, there was no guarding or rebound tenderness. Nasogastric tube was inserted and 400 cc of feculent material drained. His blood investigations revealed total white blood count of 14.3 × 109/l, lactate 5, urea 10.6 mmol/l and creatinine 119 μmol/l. Arterial blood gas showed a compensated metabolic acidosis with pH 7.36, bicarbonate 20.4 mmol/l and base excess −4.4. Abdominal X-ray showed dilated small bowel (Fig. 1), and contrast-enhanced computed tomography (CT) of the abdomen showed dilated small bowel with transition point at distal ileum. There was circumferential wall thickening at left iliac fossa. After 1 l of fluid resuscitation, repeated lactate remained raised at 5.5, which raised the concern of bowel ischaemia. Thus, emergency exploratory laparotomy was performed. Intraoperatively, an intraluminal mass was noted 7 cm proximal from the terminal ileum (Fig. 2). An enterotomy was done and revealed a piece of mushroom (Fig. 3). Retrospectively, upon further questioning, patient had poor dentition and had swallowed a mushroom 6 days ago on Chinese New Year Eve when family members from near and far gather for a reunion dinner.

Dilated small bowel with collapsed large bowel.
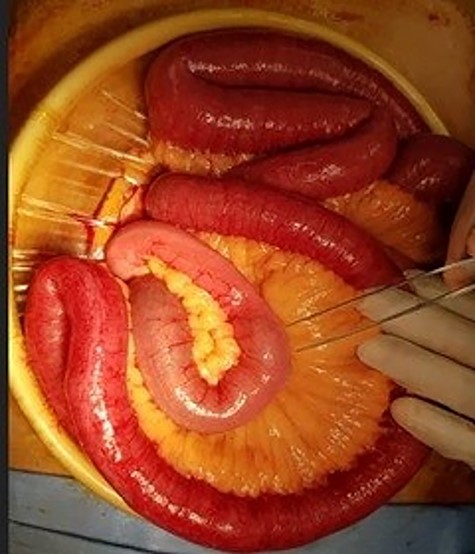
Intraluminal mass found in distal ileum.

Partially cut shiitake mushroom retrieved at enterotomy.
SECOND CASE
After 5 days, a 61-year-old Indian gentleman presented with generalized abdominal pain and vomiting for 5 days. On examination, his abdomen was distended, but soft and non-tender. CT abdomen revealed dilated small bowel with a suspicious mass at the ileum (Fig. 4). He denied neither swallowing any foreign body nor mushroom. Nasogastric decompression was done, but his condition did not improve with conservative measures. He underwent exploratory laparotomy where an intraluminal mass was found 160 cm from the terminal ileum with collapsed bowel distally. An enterotomy was done and an uncut mushroom was found (Fig. 5). Later on, he recalled that he had indeed consumed a piece of Chinese mushroom 7 days prior to admission.

CT scan showing a suspicious mass at the distal ileum of the second patient.

An uncut whole piece of shiitake mushroom retrieved in the second patient.
DISCUSSION
Phytobezoars are aggregates of indigestible vegetables or fibres in the gastrointestinal tract. It is an uncommon, albeit well documented cause of small bowel obstruction. Savaş et al. [3] reported 14 (3.2%) cases of small bowel obstruction caused by phytobezoars out of 432 cases of small bowel obstruction treated within 10 years. The reported foods that cause phytobezoars include celery, pumpkin, grape skin, prune, raisin, persimmon, broccoli and potato [4, 5]. These foods contain high amounts of indigestible fibres such as cellulose, hemicellulose, lignin and tannins. When consumed in large amounts, the tannic acid in these foods is transformed from its monomeric form to a tannin–cellulose–protein complex by gastric acid. This complex then forms a concrete-like viscous mass that conglomerates in the gastrointestinal lumen [6].
Shiitake mushroom (Lentinus edodes) is a rare cause of phytobezoars that results in intestinal obstruction [2]. It is commonly served in Chinese cuisines in Asian countries, especially during the Chinese New Year festive season and is widely available in most Asian grocery stores. It has also long been used in traditional Chinese medicine, whereby its consumption was recommended for longevity and good health [7]. Commonly sautéed or added to soups, the mushroom becomes soft in consistency and is commonly served whole or partially sliced in East Asian dishes. The mushroom is composed of 49.1% fibre, 82.9% of which is insoluble fibre. Due to its rich source of insoluble fibre, digestion may be difficult, and this may lead to luminal obstruction if a large piece of the mushroom is ingested [8].
Previous gastric surgery, poor mastication, ingestion of high-fibre food, diminished gastric secretion and motility as well as diabetic neuropathy have been reported as predisposing factors for phytobezoar formations [3, 4]. Both our patients had no previous abdominal surgery or medical illness that may impair intestinal motility. However, the first patient was edentulous and indeed swallowed a partially sliced mushroom 6 days before the presentation. The second patient, despite normal dentition, had not adequately chewed the mushroom 7 days prior to admission. In a separate case series of intestinal obstruction caused by shiitake mushroom reported by Jinfu et al. [8], both patients were edentulous and had not put on their dentures for mastication. The shiitake mushroom has a soft and slippery texture, making it susceptible to accidental ingestion without proper chewing.
The mainstay of management of intestinal obstruction due to phytobezoars is surgery. Intraoperatively, the phytobezoars are usually found in terminal ileum and jejunum. Enterotomy with extirpation of the bezoar is usually performed and segmental resection may be needed in cases of bowel ischaemia or bowel wall necrosis resulting from the bezoar. Alternatively, crushing the phytobezoars and passing the contents through the caecum without enterotomy can also be performed [9]. Laparoscopic surgery is also increasingly performed for the treatment of phytobezoars. Zeki and Okan [9] reported successful laparoscopic surgery in 12 patients with two cases requiring conversion to laparotomy.
In one of the cases of mushroom bezoar reported by Jinfu et al. [8], the preoperative CT scan showed small bowel obstruction secondary to a non-uniform foreign body. The patient underwent successful laparoscopic exploration and enterotomy to remove the mushroom. Endoscopic treatment of shiitake mushroom bezoar has also been reported in the literature. Meiko et al. [10] reported the endoscopic treatment for a patient with jejunum obstruction due to shiitake mushroom. Double-balloon endoscopy was performed and the mushroom was crushed and cut with a snare. Abdominal X-ray performed later showed that the mushroom has migrated to the descending colon. The prerequisites for endoscopic treatment were the correct cause and site of bowel obstruction. In this patient, diagnosis of jejunum obstruction due to shiitake mushroom was able to be made due to CT images that strongly suggest a mushroom and a convincing history of recent shiitake mushroom ingestion.
In our case series, both patients presented with acute small bowel obstruction with unclear cause of obstruction. Nevertheless, surgery was needed due to concerns of impending bowel ischaemia and failure of conservative management, respectively. Retrospectively, there are two important take-home messages. First, phytobezoars should be suspected in elderly edentulous patients. Second, dietary history is an important clue to the possible cause of obstruction in patients without prior abdominal surgery. Shiitake mushroom should be kept in mind as a possible cause of phytobezoars, especially during the Chinese New Year festive season when its consumption is tremendously increased.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}