





Abstract
Fibrous dysplasia is a rare condition. We present a case of a 34-years-old man presented with left-sided facial pain, headache and nasal obstruction for a long duration. CT scan of the sinuses showed a mass occupying the left ethmoidal region abutting the orbit and skull base obstructing the left frontal sinus. The patient was treated successfully by image-guided endoscopic endonasal removal of the tumor with no recurrence after 3 years of follow-up. This report aims to show the usefulness of endoscopic endonasal removal of a large fibrous dysplasia of paranasal sinuses and skull base.
INTRODUCTION
Fibro-osseous benign lesions rarely affect the sinonasal tract, and are divided into three different entities, namely osteoma, fibrous dysplasia and ossifying fibroma. Osteoma is the most common benign tumor of the nose and paranasal sinuses [1], and the frontal sinus is its most frequent location (70–80%), followed by the ethmoid, maxillary and sphenoid sinuses in descending order [2]. Most osteomas are simple exostoses, which are probably malformations rather than true tumors. Ossifying fibroma is considered to be a rare benign fibro-osseous lesion, most commonly seen in women in the third and fourth decades of life [3]. It consists mainly of the mandibular and maxillary bones, although it can rarely develop in the nasal cavity [4]. Fibrous dysplasia is a benign, slowly progressing dysplastic process of altered osteogenesis, in which the normal medullary bone is replaced by the abnormal fibro-osseous tissue that may occur within a single or multiple bones. Rather than a true neoplasm, the disease can be regarded as a developmental anomaly, in which the normal medullary space of the affected bone is progressively replaced by disorganized fibro-osseous tissue.
CASE REPORT
A 34-years-old man presented with left-sided facial pain, headache and nasal obstruction for a long duration, with no history of bleeding per nose, nor blurring of vision. Upon examination, there was a large left nasal cavity bony outgrowth pushing the middle turbinate and pushing the nasal septum to the right side (Fig. 1). CT scan of the paranasal sinuses showed a large mass centered in the left anterior ethmoid sinus, the mass measures 3.7 × 2.9 cm (trans-axial) (Fig. 2) and 3.7 × 5.2 cm (coronal) (Fig. 3), it has a heterogeneous density with calcified and soft-tissue component. The calcified component is in the periphery with central soft tissue density. The mass resulted in remodeling of adjacent bones with nasal septal deviation to the right, it extended superiorly to involve the frontal sinuses as well as invading the left cribriform plate and intracranial extension (Fig. 4), it extended inferiorly displacing the medial wall of the left maxillary antrum. The medial aspect of the mass caused remodeling of the medial wall of the left orbital cavity with bulging and displacement of the medial rectus muscle. The mass resulted in obstruction of the left frontal sinus.
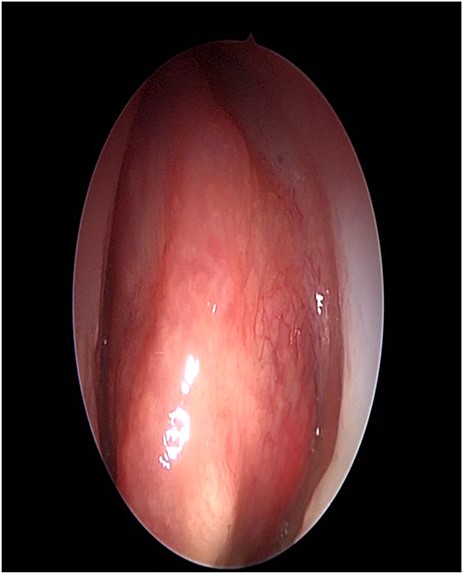
Nasal endoscopy image showing a bony mass attached to the left middle turbinate pushing the septum to the right.
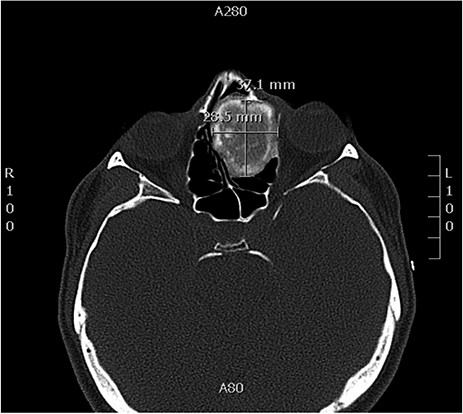
Axial CT image of the sinuses showing a mass filling the left ethmoidal sinus.
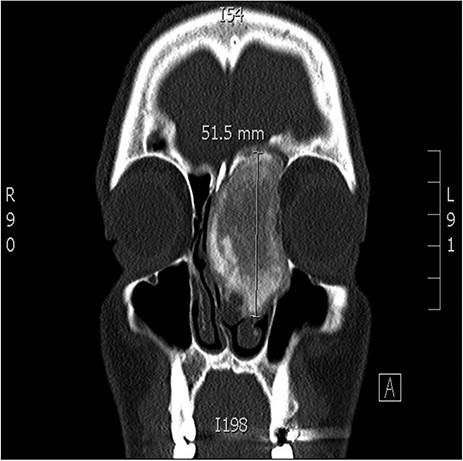
Coronal CT image of the sinuses showing a large mass obstructing the frontal sinus.
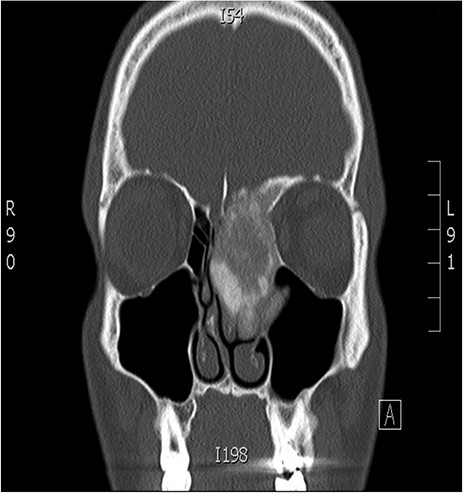
Coronal CT image of the sinuses showing a mass encroaching the orbit and skull base.
The patient underwent image-guided endoscopic endo-nasal removal (Fig. 5) of a large fibro-osseous tumor, the tumor was adherent to the orbit and skull base which was removed (Fig. 6). The resected tumor was sent to the histopathological examination, which confirmed the final diagnosis of fibrous dysplasia. The patient remained free of symptoms with no recurrence for 3 years after the resection.

Image-guided endoscopic tumor removal from orbit and skull base.
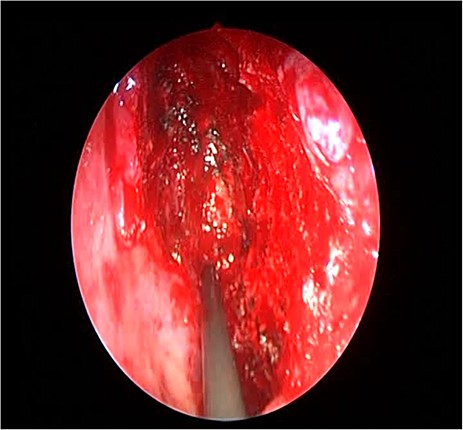
Endoscopic image showing the cavity after tumor removal from the orbit and skull base.
DISCUSSION
This report presents our experience in the management of symptomatic fibrous dysplasia of the paranasal sinuses and the skull base. The outcome was auspicious with the majority of patient symptoms amended after surgical treatment. The endo-nasal endoscopic approach with image guidance was the main approach performed to substantiate the diagnosis and to abstract the tumors from the sinuses, orbit and the skull base. Fibrous dysplasia is an unusual, non-familial bony disorder that is often a deforming and devastating condition affecting both sexes equally [5]. It has traditionally been regarded as a disease of childhood, and some ascendant entities believed the disease to be quiescent after puberty. However, at present, the emerging concept seems to be that fibrous dysplasia may progress to adulthood [6]. It is an eccentric proliferation and differentiation of bone marrow stromal cells, engendering exorbitant fibrous tissue within the bone marrow [7]. The relegation system subdivides the disease into three types: type 1, is monostotic and characterized by unique or multiple lesions in a single bone, type 2, is polyostotic and, characterized by multiple lesions involving different bones and type 3, is characterized by dissemination of pathological bone changes connected to other protuberances such as McCune–Albright syndrome (polyostotic fibrous dysplasia, cutaneous pigmentation and endocrine abnormalities) [8]. Monostotic fibrous dysplasia is the most prevalent form (80%), with prevalent involution of the ribs and femur, and 20% of cases are localized in the head and neck region [2,7]. Polyostotic fibrous dysplasia, which overall accounts for 20% of cases [2]. With fibrous dysplasia, the bone grows in the form of a pain-free swelling, while the maxilla and mandible are most frequently involved in the head–neck zone, the ethmoid bone is infrequently involved. Malignant transformation is recherché (0.5%), and is customarily visually perceived only in polyostotic cases [8]. CT scan has proved most subsidiary in detecting and defining fibrous dysplasia lesions of the cranial base. CT scan is excellent for assessment of the bulk and morphology of tumors and may be more auxiliary in determining the extent of bony involution. Magnetic resonance imaging offers more preponderant specificity in neurovascular and ocular involution [9]. A ground-glass appearance on CT scans, thinning of the cortical bone and ballooning of the affected area are the hallmarks and special features of fibrous dysplasia [10]. Surgery is indicated in most cases of consequential cosmetic deformity or complications such as visual problems. This is customarily accomplished via an endonasal endoscopic tumor removal. The advantages of endoscopic endonasal procedures are minimally invasive technique, fewer morbidities, accurate localization, shorter hospital stay and avoidance of the external scars of the open surgical procedures. Patients should be followed up with endoscopic examination and periodic imaging if indicated to guide the management of any recurrence.
CONCLUSION
Fibrous dysplasia is a rare condition. We report a patient with left facial pain, headache and nasal obstruction. CT scan showed a fibro-osseous mass occupying the left ethmoid with obstruction of the left frontal sinus invading the orbit and skull base, treated successfully by image-guided endonasal endoscopic removal of the tumor with no recurrence after 3 years of follow-up. This case shows the usefulness of image-guided endonasal endoscopic sinus surgery in the treatment of fibrous dysplasia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}