





Abstract
The majority of patients with renal cell carcinoma develop recurrence within 5 years following radical nephrectomy. Very late sole local recurrence beyond 10 years is rare, and all reported cases had clear cell histology. Surgical resection of local recurrence remains the best option for disease management. This case opens the way for further studying the rare histological variants of renal cancer and to encourage prolonged follow-up and offering surgery as the best option for managing these cases.
INTRODUCTION
Follow-up for patients with T1 renal cell carcinoma (RCC) is variable in different guidelines. American guidelines recommend yearly radiological surveillance for 3 years [1], while Canadian guidelines recommend radiological surveillance at 2 and 5 years after surgery [2]. European Association of Urology guidelines recommend yearly radiological surveillance for 3 years then every 2 years with patients counselling [3]. Although the interval of follow-up was variable, they all agreed on short follow-up of 3–5 years, with only optional extended follow-up through the European guidelines.
Park et al.[4] studied factors associated with late recurrence following radical nephrectomy (RN) and found that all late recurrence beyond 5 years had clear cell histology except a single patient who had chromophobe histology. Noguchi et al.[5] did a retrospective study of 1398 patients managed surgically for localized RCC and found that 100% of >5-year recurrence was of clear cell histology.
CASE REPORT
We were encountered with 57-year-old lady complaining of left dull aching loin pain. Examination revealed a palpable mass in the left loin. She gave a history of left RN 15 years ago, and pathology report showed T1b chromophobe RCC (chRCC) with negative resection margin. She was followed for 5 years before being discharged from oncological surveillance. Computed tomography (CT) of the abdomen and pelvis was requested and showed large (13 × 11 × 11 cm3) heterogeneous enhanced mass, occupying left renal bed (Fig. 1). CT of the chest was free of metastases. CT-guided biopsy was done, and pathology was favouring chRCC.
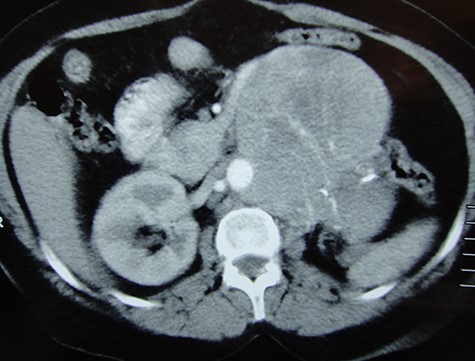
CT scan coronal image showing a large recurrence in left renal bed.
The patient was counselled, and surgery was successfully done through a generous chevron incision. Fig. 2 shows the resected tumour. Final pathology confirmed the diagnosis of chRCC. The patient recovered well from surgery with no intraoperative or early postoperative significant complications.

The mass following complete resection.
To our best knowledge, this is the first case in literature, reporting a very late sole local huge recurrence of chRCC. Patient’s consent for publishing was obtained, and no identifier data were included in the study.
DISCUSSION
chRCC is an uncommon pathological variant that tend to present as a single mass, usually with no extension beyond renal capsule and no venous or sinus infiltration. A review article found that the progression-free survival of a low grade at 5 year to be 100% [6]. Abara et al.[7] reported three cases that recurred >10 years post-RN. The three patients had clear cell histology, and only one patient had local recurrence, while the other two had recurrence in the contralateral kidney or as a lung mass.
Our case is unique, describing 15-year local recurrence of a huge mass of chRCC. Metastatic workup confirmed the sole local recurrence. The patient was counselled about the high surgical risk and fortunately had a safe open surgery, with no Clavien Grade 3 or higher complications. Long follow-up will be scheduled for this patient to prove good response with no further local or distant recurrence.
In agreement with our surgical decision, a recent review article confirmed that surgery for local recurrence should be prioritized whenever feasible over systemic treatment [8]. Herout et al.[9] retrospectively identified 54 patients with local recurrence following RN and concluded that patients with disease-free survival longer than 2 years before developing local recurrence tend to have good survival following local resection.
CONCLUSION
chRCC can rarely show very late recurrence, and prolonged surveillance is recommended following RN, regardless of the histological type. Surgical management is feasible for local recurrence and should be attempted whenever possible.
Acknowledgements
We would like to acknowledge the great role of our operating nursing staff that was highly trained and efficient to allow safe successful surgery.
Conflict of Interest
No conflict of interest from all authors.
Funding
No source of funding.

{kind=link}
{kind=link}