





Abstract
BCG is a well-established treatment for superficial bladder cancer. Although usually well-tolerated, side effects can range from mild cystitis to life-threatening sepsis. Epididymitis is a rare complication of BCG, with only a handful of cases proven to be caused directly by Mycobacterium bovis. We describe one such case, along with radiological findings for this rare complication.
INTRODUCTION
Intravesical Bacillus Calmette-Guérin (BCG) is a long established and proven therapy for treatment and prevention of G2T1 and G3 Ta/T1 bladder transitional cell carcinoma (TCC) and carcinoma in situ (CIS). Although generally well tolerated, complications of having been reported, ranging from cystitis, myalgia and pyrexia to life threatening and fatal sepsis [1]. Tuberculous-epididymitis following intravesical BCG has only been reported in a handful of cases. We describe one such case, along with radiological findings and a review of the literature for this rare complication.
CASE REPORT
A 73-year-old patient with a history of previous transurethral resection (TUR) of the prostate, presented with dysuria and urinary infection and was found to have an intravesical lesion on flexible cystoscopy. As part of his work up, a CT urogram was performed but no upper tract abnormalities were detected. He underwent TUR for this lesion which histological analysis revealed to be a G3 pT1 bladder TCC. Subsequent cystoscopy and re-resection showed further G3 pT1 disease and CIS.
To prevent further recurrence, the patient was offered adjuvant intravesical BCG immunotherapy, and he completed a 6-week course of treatment without complication. He was followed up after completing this course of BCG with flexible cystoscopy, which showed only generalized inflammation but no recurrence.
Three months later, a further 3-dose maintenance course of intravesical BCG was given, after which the patient began experience right sided testicular pain and swelling. He was treated for epididymitis with a prolonged course of oral antibiotics and anti-inflammatory medication.
At a further check cystoscopy 1 month later, it was noted the patient continued to have right scrotal swelling and pain, as well as pus extruding from a sinus in the scrotal skin. Ultrasound scanning of the scrotum revealed a heterogenous focus of tissue calcification within the right epididymal tail, and inflammatory changes associated with granulomatous change (Fig. 1a and b).
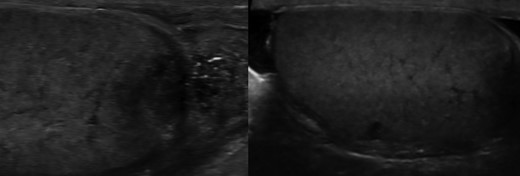
a) and (b) Ultrasound scan showing heterogeneous focus of tissue calcification within the right epididymis and granulomatous change.
A pus swab yielded a negative result for acid fast bacilli under microscopy, but a positive result for Mycobacterium bovis variant using whole genome sequencing. He was subsequently commenced on a 6 month course of isoniazid, rifampicin and ethambutol as guided by antibiotic sensitivities, and referred to a local infectious diseases unit.
DISCUSSION
The first human BCG vaccine was introduced in 1921, originating from a strain of the attenuated live bovine tuberculosis bacillus, Mycobacterium bovis. Initially a vaccine for the prevention of tuberculous, BCG immunotherapy use was furthered in 1977, when it was first introduced as a treatment for non-muscle invasive bladder cancer [2]. By 2014, there were over eight considered variants and strains of live attenuated Mycobacterium bovis used for intravesical immunotherapy [2]. Though the mechanism is not fully understood, instilled mycobacteria are thought to provoke a local immune reaction that causes destruction of tumour cells.
Side effects of BCG immunotherapy are well documented ranging from mild symptoms of cystitis, low grade pyrexia and myalgia, to life threatening and fatal sepsis [1]. Epididymitis is uncommon following intravesical BCG immunotherapy, occurring in around 0.4% of patients [1]. To the best of our knowledge, there are only 13 cases in literature of epididymis-orchitis caused directly by BCG immunotherapy [3–5].
Of clinical importance is the differentiation between tuberculous-epididymitis and other bacterial pathogens following intravesical BCG treatment. Clinical features of dysuria, scrotal pain and swelling with or without pyrexia are usually present in both pathologies, however ultrasonography may provide some clues [3].
Various patterns of tuberculosis epididymitis and orchitis have been described, including diffuse hypoechoic heterogeneous enlargement, diffuse hypoechoic homogeneous enlargement, and nodular hypoechoic heterogeneous enlargement [6]. If present, as in our case, heterogenenic appearances are thought to result from the various stages of granuloma formation in response to mycobacterium infection [3]. Other features of tuberculous-epididymitis include hydrocele, cutaneous swelling, extratesticular intrascrotal calcifications, abscesses, and scrotal sinus tract [7].
The radiological differentiation between tuberculous-epididymitis, testicular malignancy and torsion can be a diagnostic challenge. Although testicular torsion in its chronic phase will produce similar heterogeneity, on doppler USS there will usually be a demonstrable avascularity present in the affected testis, as compared with hyperaemia in early orchitis [3].
Demers and Pelsser point out that heterogeneity in testicular malignancy is not usually accompanied by epididymal enlargement in the early stages until there is direct extension of tumour [3]. Commonly, other cases in the literature have described diagnosis through histological analysis following orchidectomy, where testicular malignancy was suspected [4]. Some have advocated the use of biopsy prior to orchidecomy in cases where tuberculous-epididymitis forms part of any differential diagnosis [3].
Post BCG-immunotherapy infections can vary widely in their presentation and incubation. Clinicians should have a high index of suspicion in any patient with infective symptoms, especially those who fail to respond to conventional antibiotics.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}