





Abstract
Hydatid disease is caused by a tape worm Echinococcus Granulosus that lives in the intestines of the definitive host which is the dog or other carnivore. Human is the accidental intermediate host and become infected by ingesting contaminated vegetables or water with the eggs of the parasite.
A-37-year old male presented with right side abdominal pain for 2 months. Abdominal examination showed a large right side abdominal mass extending from the right subcostal region to the right iliac fossa. CT-scan showed two cystic lesions in the right lobe of the and a third one extending to the pelvis. During surgery aspiration of 10 liters of bile stained fluid done. Excision of the cysts done. Tube drain put inside the cyst cavity with omentoplasty. There was bile leak to the drain which stopped over one month. The patient received anthelminthic medication for 3 months.
INTRODUCTION
Hydatid disease is a zoonotic disease that is present worldwide. The disease is caused by a tape worm, human infection occurs by tow main types: Echinococcus Granulosus and, less commonly, Echinococcus Multilocularis [1].
The parasite is a hermaphrodite, the adult form range between 4-6 mm in length which lives in the intestines of the definitive host which is the dog or other carnivore. It is attached to the mucosa of the intestine by the mean of hooklets, the terminal segment e which is called the gravid proglottid contains large number of eggs which are passed with the feces [1].
When the intermediate host; which is either the sheep or other ruminant; ingest the eggs the embryo is released and passed through the portal venous system or the lymphatics to involve almost any organ. The live cycle is completed when the viscera of an infected intermediate host which contain the larval stage are ingested by the definitive host. Human become infected when he ingests contaminated vegetables or water with the eggs of the parasite or by close contact with infected definitive host [1].
CASE PRESENTATION
A-37-year old male presented with right side abdominal pain for 2 months.
The pain was dull in nature, with no aggravating and relieving factors, there were no associated symptoms. The patient had non relevant past medical and surgical history.
During examination; the patient had normal vital signs and no findings detected on general examination. Abdominal examination showed a visible large bulging mass in the right side of the abdomen extending from the right subcostal region to the right iliac fossa, which was firm in consistency, non-tender, and smooth surface, Fig. 1.

Showing a bulging mass in the right side of the abdomen.
The biochemical tests were normal including the serum bilirubin level and liver enzymes. CT-scan of the abdomen showed two non-enhancing cystic lesions in the right lobe of the liver 11 cm and 10 cm containing undulating membrane (water-lily sign), and a third large cyst extending to the pelvic cavity 40 cm in length (features of multiple hydatid cyst of the liver), Fig. 2.
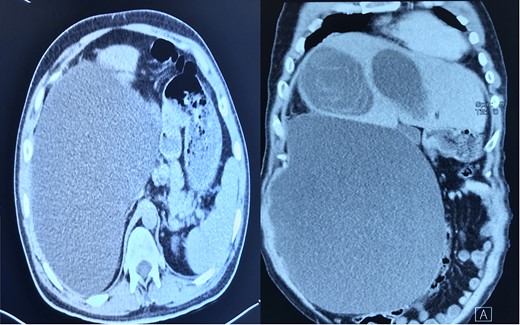
CT-scan of the abdomen showing three large cystic lesions related to the right lobe of the liver.
During surgery through a midline laparotomy, isolation of the cyst done with packs soaked with chlorhexidine solution to prevent contamination of the wound and the abdominal cavity with the cyst fluid, aspiration of six liters of bile stained fluid done at the first instance, Fig. 3.

Intra-operative picture showing isolation of the cyst and initial aspiration of six liters of bile stained fluid.
The cyst mobilized outside the abdominal cavity, and further four liters of the fluid aspirated, Fig. 4.
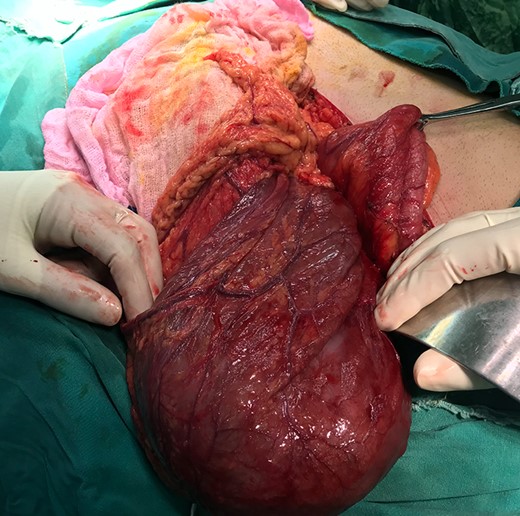
Intra-operative picture showing huge cyst mobilized outside the abdominal cavity.
The cyst found to be connected by a narrow pedicle to the edge of the right lobe of the liver, Fig. 5.
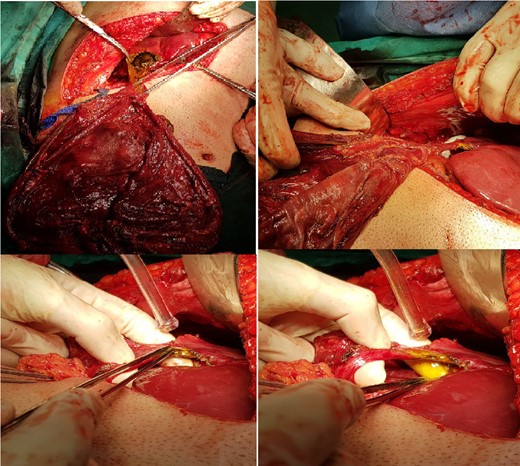
Intra-operative picture showing the cyst connected by a narrow pedicle to the right lobe of the liver.
Excision of the cyst done with extraction of the other two cysts from the cyst in the liver parenchyma, two small bile canals detected connected to the cyst cavity which then sutured with 3/0 slowly absorbable monofilament suture material, Fig. 6.
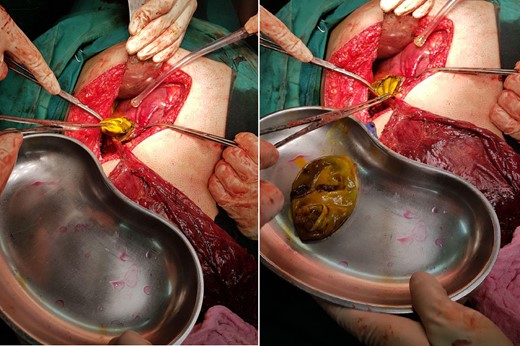
Intra-operative picture showing extraction of two laminated membrane of the hydatid cyst from the liver.
Tube drain put inside the cyst cavity with omentoplasty and the patient discharged 6 days after the surgery. There was bile leak to the drain which stopped gradually over one month. The patient received anthelminthic medication for 3 months.
DISCUSSION
The hydatid cyst consists of three layers, the outer layer composed of compressed host tissue and the other two inner layers are formed by the parasite tissue. The inner two layers are the laminated membrane which forms the first layer, it is whitish in color, acellular and about 2-3 mm thick and allows the passage nutrient material to the inside of the cyst. The innermost layer called the germinal layer, is very thin and translucent, it produces the laminated membrane and forms the scolices of the parasite. These scolices if detached from the germinal layer and become floating in the cyst fluid called the hydatid sand.
The liver is the most common organ involved, followed by the lungs, and almost any other organs could be affected to lesser extent [1, 2].
The disease can present with a variety of clinical presentations depending on the organ involved, the size of the cyst and the development of complications. Hydatid cyst of the liver usually present with right upper quadrant pain, obstructive jaundice from intra-biliary rupture or compression from outside, or emergency presentation like intra-abdominal rupture, anaphylaxis, or even death [2, 3].
The cyst could be diagnosed incidentally in some cases during workup for some other diseases, usually the cyst is diagnosed by ultrasound, CT-scan and MRI will show more detailed information about the organs involved, presence of complications and the consistency of the cyst contents like the presence of clear fluid, hydatid sand, floating membrane, or daughter cysts or calcifications in the wall of the cyst. MRI more useful for the cyst involving the brain or detecting complicated cyst as connection with the biliary system [4, 5].
Medical treatment may be used with anthelminthic drugs which had been shown to be effective especially for uncomplicated cases [6].
Operative treatment is essential in most of the cases. The intervention is either by laparoscopic surgery of the open approach. There are many surgical options of treatment depending on the diseases and the surgeon experience like cyst evacuation, marsupialization, excision, omentoplasty or filling the cavity with normal saline, anastomosis with the intestine like cyst-jejunostomy or cyst-gastrostomy may be done when major connection is found with the biliary tree depending on the site of the cyst. Radical surgery with complete excision of the affected segment can be done safely in some cases [1, 7, 8].
Percutaneous aspiration under radiological guide and sterilization of the cyst by injection of scolicidal agent may also be tried with variable response, it may be combined with anthelminthic drugs in selected patients [3, 7].
Complications may occur during surgery or after that which may result from prolong hospital stay or readmission, anaphylaxis may occur during surgery due to spillage of the cyst contents which cause allergic reaction, bleeding and hematoma may occur, prolong tube drainage, infection in the residual cavity, cholangitis, biliary-cutaneous fistula, omentoplasty had been shown to be associated with lower rate of local complications [1, 9, 10].
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
The authors are the source of the funding.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}