





Abstract
Ovarian cancer (OC) is one of the most commonly diagnosed cancers among women. Regretfully due to its a broad spectrum of clinical behavior and challenging diagnosis most cases are diagnosed at a late stage. On rare occasions, these tumors can grow to massive sizes if left untreated, worsening the prognosis of the patient. Thanks to the advancement of medicine and diagnostic techniques, these rare cases are less frequent. Timely detection and surgery could avoid all these potentially troublesome scenarios. We report the case of a 64-year-old female with a giant 13 kg high-grade papillary serous ovarian cystadenocarcinoma, the tumor grew during a four year period and was adequately treated with surgery and is under close follow up with the oncologist. To our knowledge, this is the first case of a giant ovarian cystadenocarcinoma ever reported in Ecuador.
INTRODUCTION
In recent years, huge ovarian tumors have become extremely rare in the current medical practice, as the majority of cases are diagnosed early during routine gynecological examinations or as incidental findings [1, 2]. However, when they occur these rare ovarian tumors can endanger the patient’s life not only because of their risk of malignancy but because they can cause several complications due to their size [1, 3]. We report the case of a 64-year-old female with a giant 13 kg high-grade papillary serous ovarian cystadenocarcinoma that grew over a period of 4 years.
CASE REPORT
Patient is a 64-year-old female with a past medical history of hysterectomy and a right oophorectomy. She presented to our department with a four-year history of abdominal mass in her lower abdomen that has grown to gigantic proportions, however, due to a lack of adequate access to healthcare facilities and a fear of a possible surgery caused her to not seek any medical attention. Nonetheless, in the previous 4 months, she noticed pain around the mass, severe weight loss and recurrent episodes of postprandial vomit. On clinical examination a 40 × 34 cm hard, nontender abdominal mass was found in her abdomen, (Fig. 1A) the tumor was hard in consistency, and non-mobile. Auscultation of the abdomen revealed normal bowel sounds. Laboratory data including were normal, however CA-125 was slightly elevated.
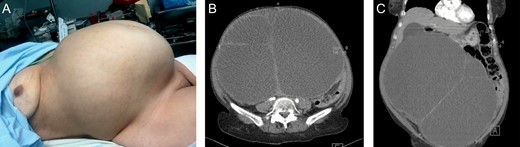
A: Giant abdominal mass. B: Contrast-enhanced CT: Giant mass with heterogeneous contrast enhancement on its wall, and filled with a heterogeneous fluid. C: Contrast-enhanced CT: Giant mass, that displaced most of the abdominal contents.
A contrast-enhanced computed tomography (CT), revealed a 32 × 34 × 29 cm, giant mass with heterogeneous contrast enhancement on its wall, it was filled with a heterogeneous fluid and solid peripheral zones with some calcifications, it appeared to arise from the left adnexa and it displaced most of the abdominal contents. Yet, it did not invade any adjacent structures and no other masses were observed. (Fig. 1B and C)
With these findings, surgery was decided, at a laparotomy a huge 32 × 34 × 30 cm ovarian tumor was found, it had gray walls and was completely surrounded by the omentum. It was attached to the mesentery of the small bowel and the left adnexa. No other masses, or lymph nodes or were encountered. (Fig. 2A–C) From there the surgical decision was straightforward and complete excision of the mass without spillage or spread was performed. Due to the size of the mass and the fact that malignancy was suspected a complete resection along with an appendectomy and omentectomy was completed, without complications
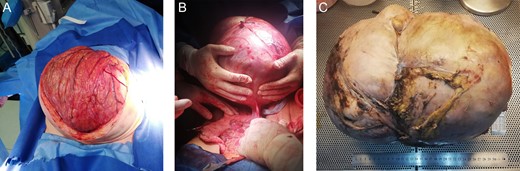
(A) Surgery, Giant ovarian mass covered by omentum. (B) Resection of the ovarian mass from adhesions to the bowel. (C) Completely resected tumor.
Pathology reported a giant 13 kg high-grade papillary serous ovarian cystadenocarcinoma, its capsule had multiples necrosis patches and measured 15 to 25 mm on average. It had a huge cavity that contained about four liters of a brown mucous liquid. Regretfully the tumor had an appendiceal an omental extension. (Fig. 3A–C)
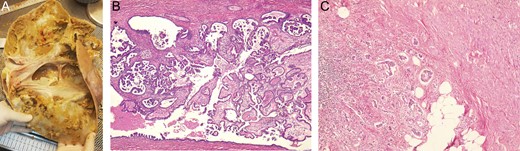
(A) Tumor had macroscopically visible papillary vegetations on the inside of the cyst wall. (B) Microscopy revealed ovarian stroma with atypical cells. (C) Appendiceal wall, invaded by atypical cells ovarian tissue.
The postoperative period of the patient was uneventful, on the second postoperative sips of liquids were initiated. Attaining good oral tolerance, a soft diet was initiated. The patient was discharged in good conditions. On follow-up controls, the patient is doing well and is undergoing periodic controls with an oncology specialist.
DISCUSSION
OC is the seventh most commonly diagnosed cancer among women in the world [1]. There are many genetic abnormalities and several reproductive and hormonal factors that have been related to an increased risk of developing this kind of cancer. Regretfully this disease is usually diagnosed at a late stage when the 5-year survival rate is only 29% [1, 4]. Over 90% of ovarian cancers can be classified in five subtypes: high-grade serous, low-grade serous, mucinous, endometrioid, and clear-cell carcinoma [4]. OC usually affect women around 60 years old and has a broad spectrum of clinical symptoms. Patients may be completely asymptomatic in early stages, however abdominal fullness, dyspepsia, early satiety, bloating, ascites or abdominal masses can appear as the disease progress [1, 3]. Due to this, OC should be considered in any premenopausal woman with an unexplained enlargement of the ovary or any postmenopausal woman with a palpable ovary or mass [1]. Ovarian masses are considered large if they have diameters between 5 and 15 cm, when they are bigger than 20 cm they are usually named giant. The largest tumor of the ovary weighed 137.4 kg and was completely removed by O’Hanlan in 1994. Since then, the incidence of giant ovarian masses has declined due to the advancement in medical information and easier access to health-care [2, 5]. Nonetheless, rare cases such as ours can still occur.
Complementary exams are needed to confirm the diagnosis, a transvaginal ultrasound is often performed to evaluate the pelvis, nonetheless, a CT can provide more detailed information about an ovarian mass. CA-125 levels can also be used as it is elevated in more than 80% of patients with epithelial OC nonetheless it is not sufficiently sensitive nor specific enough to be diagnostic [3, 4]. As it was found in our patient.
If doubt persists exploratory surgery either with a laparoscopic or conventional approach is an essential part of the investigation for a patient [1]. Masses less than 8 cm in a premenopausal woman and less than 5 cm in a postmenopausal woman can be conservatively managed, however giant ones require resection because of their symptoms due to their size such as a respiratory compromise or abdominal pain and their inherent risk of malignancy [5, 6]. Complete resection without injuring the bowel or other organs along with prevention of spillage of the cyst fluid into the cavity, either with a laparoscopic or open approach, must be achieved [1, 2, 7]. In our case, due to the history of the patient, and the size of the mass, laparotomy was decided and the tumor was completely resected, without complications.
Histologic confirmation is necessary as other causes of ovarian diseases including a complex ovarian cyst, metastatic diseases or benign conditions, can generate giant ovarian masses [1, 3, 4]. Despite successful surgery, most patients will require chemotherapy as it improves survival [4]. As our patient encountered.
OC will continue to be a risk for woman, as the majority of patients will be diagnosed at a late stage. Although the incidence of giant ovarian masses has decreased worldwide, these rare cases can still occur. This case proved that adequate healthcare services along with a high clinical awareness by all physicians are vital when approaching an ovarian mass, also in a unique way it showed us that even in giant abdominal masses a careful dissection is necessary to avoid complications and to improve the patient’s prognosis.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}