





Abstract
Sexual activity is unlikely to result in spinal injuries. We present the first case of a cervical fracture-subluxation and spinal cord injury following sexual activity. This 31-year-old female presented to the emergency room with neck pain and quadriparesis, following sexual activity in an extreme position. Imaging revealed a hyperflexion cervical fracture-subluxation injury, requiring reduction by traction, followed by circumferential surgical fixation. At 6 months postoperatively, she reported baseline return of function. This case demonstrates that sex-induced spinal injuries are possible and may require urgent surgical treatment.
INTRODUCTION
Sexual activity may result in significant untoward effects, such as myocardial infarction and penile fractures [1, 2]. Patients with low back pain may also suffer episodes of acutization during or after intercourse [3, 4]. However, to our knowledge, there have been no reports of significant spine and spinal cord injuries as a direct result of sexual activity. Here, we report the first case of a cervical spinal fracture-subluxation, with resultant spinal cord injury, induced by extreme sexual activity.
CASE REPORT
A 31-year-old African American female reported to the Emergency Department for complaints of neck pain and generalized weakness. The pain started suddenly, following neck hyperflexion during sexual activity with her significant other. The patient reported being in an unusual position, resting the back of her head against the floor, with the neck in hyperflexed position, and the torso and lower body up in the air, supported by her significant other. Upon forced hyperflexion, the patient felt a ‘pop’ and then immediate onset of pain and weakness. She did not lose consciousness. She reported consuming ‘a fair amount’ of alcohol prior to the event.
On arrival at the emergency room, she complained of neck pain and exquisite bilateral hand tenderness. Motor exam revealed weakness in elbow extension (American Spinal Injury Association—ASIA grade 4/5 on left, 0/5 on right), hand grip (2/5 bilaterally), and left leg (3–4/5). There was preserved bowel and bladder control. The patient was diagnosed with an incomplete spinal cord injury, ASIA C.
A computed tomography (CT) of the cervical spine without contrast revealed a C5-6 fracture dislocation and subluxation (Fig. 1) with spinal cord compression. The injury also included a posterior ligamentous complex rupture at C5-6, with fracture of the posterior lamina of C5 and right-sided jumped facet.
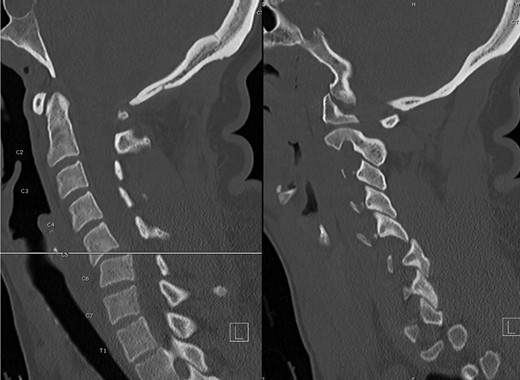
Preoperative CT, sagittal images through the center (left) and right side (right), illustrating the C5-6 fracture-subluxation and right jumped facet.
The patient’s Subaxial Cervical Spine Injury Classification (SLIC) score was 8, indicating a surgical lesion [5]. The patient was initially placed in cervical traction, with successful realignment at 30 lbs of weight. Surgical options were discussed at length with the patient, including an anterior only approach, followed by immobilization in cervical collar, versus a circumferential approach. The patient chose the latter, anticipating a more intense physical therapy for postoperative recovery. In the operating room, a singel level C5-6 anterior discectomy and fusion was initially performed, followed by a posterior approach with lateral mass screws and rods at C5 and C6. The disc was found to be severely disrupted, as expected, but no dural violation was observed. The patient had an excellent postoperative course, with immediate resolution of the hand pain and progressive return of motor function. She was transferred to the hospital’s inpatient rehabilitation center and at 2 weeks postoperatively she only exhibited trace weakness (4+/5) in the left leg and right triceps. At the 6month postoperative visit, the patient had no residual deficits and a CT-myelogram showed good incipient fusion across the disc space (Fig. 2).
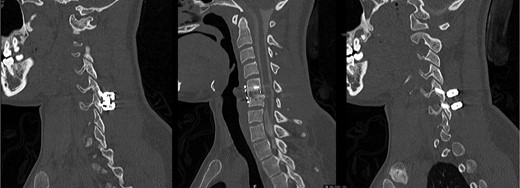
Postoperative CT-myelogram, sagittal images through the left (left), center (center) and right (right) sides, illustrating good realignment and incipient fusion at C5-6.
DISCUSSION
Traumatic cervical spine injuries are often reported in motor vehicle accidents and contact sports, such as footbal for males and horseback riding for females [6]. The degree of severity can be determined using the SLIC score [5]. Patients with a SLIC score of 5 or more are considered surgical candidates. Prompt stablization and imaging are crucial for the correct diagnosis and treatment.
The initial treatment for patients with cervical fracture-subluxation is traction, in an attempt to reduce the subluxation. This was successful in our case, obviating the need to perform an initial posterior surgical approach to reduce the slippage. The next step after reduction was to stabilize the affected spinal segment anteriorly, by performing a discectomy and fusion. Due to the high degree of instability, as well as per patient’s wishes, a final surgical step consisting in a short segment posterior fusion was performed. This allowed for the strongest segmental fixation and permitted the patient to undergo intense postoperative physical therapy, without the need for a cervical collar.
Literature regarding spinal cord injuries and sexual activity addresses mostly fertility and the capability of having sex as a complete or incomplete quadri- or paraplegic [7, 8]. We have found no reports on spinal column or spinal cord injuries directly caused by sexual activity. Therefore, it appears that this is the first case report showing that sexual activity can result in serious spine and spinal cord injuries when extreme positions are adopted.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no competing interests.
FUNDING
No funding was received for this article.
CONSENT FOR PUBLICATION
The patient consented for publication of this case report and any accompanying images.

{kind=link}
{kind=link}