





Abstract
Anaplastic thyroid carcinoma is a rare tumor, consisting 1–2% of all thyroid malignancies and presenting a high mortality rate. Median survival for patients undergoing primary surgery is approximately 6.6 months. We present a case of a patient treated with R0 resection, including total thyroidectomy and lymphadenectomy of levels III, IV, VI and VII after cervical lymph node mapping, oral 131I administration, and radiotherapy. Proper preoperative research, R0 resection and relatively early diagnosis, led to good prognosis, as the patient is currently totally disease-free, twelve months postoperatively.
INTRODUCTION
Anaplastic thyroid carcinoma (ATC) is an uncommon and aggressive thyroid tumor presenting high dedifferentiation and a disease-related mortality of almost 100%. It is more frequently diagnosed in women, and the mean age at diagnosis is 71 years. Many patients present a history of prior or coexisting goiter or differentiated carcinoma [1]. ATC has a median survival of 6 months; resistance to conventional treatment with radioiodine and thyroid-stimulating hormone suppresion contributes to this poor prognosis [2]. Recent studies show a median survival of 6.6 months in patients undergoing primary surgery, while survival in inoperable cases is 2.1 months. According to a recent review, negative margins do not seem to increase survival significantly; therefore, the extent of resection still remains controversial [3].
We present the case of a 58-year-old male patient who was diagnosed with ATC and, after lymph node mapping, submitted to total thyroidectomy and extended lymphadenectomy, radioiodine, and radiotherapy. One year postoperatively, this patient has not shown any operation-related complications or any signs of recurrence.
CASE REPORT
A 58-year-old man, diagnosed with left thyroid lobe carcinoma, was admitted to our department for further treatment. His condition was diagnosed incidentally, upon cardiologic and imaging examination during investigation of shortness of breath and fatigue. Abnormal enlargement of the left thyroid lobe due to a 7-cm node was primarily found in cervical ultrasound, as well as enlargement of multiple left cervical lymph nodes. Further imaging with cervical and thoracic computerized tomography (CT) (Fig. 1) and FNA biopsy indicated a Bethesda System сategory V neoplasia. Preoperative research also included serum calcitonin, to exclude myeloid carcinoma, and lymph node mapping (Fig. 2).
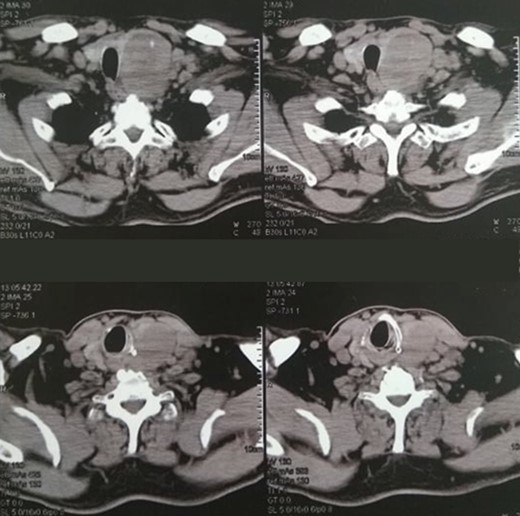
Cervical CT scan, showing a 7-cm node of the left thyroid lobe and concommitent multiple left cervical nodal enlargement.
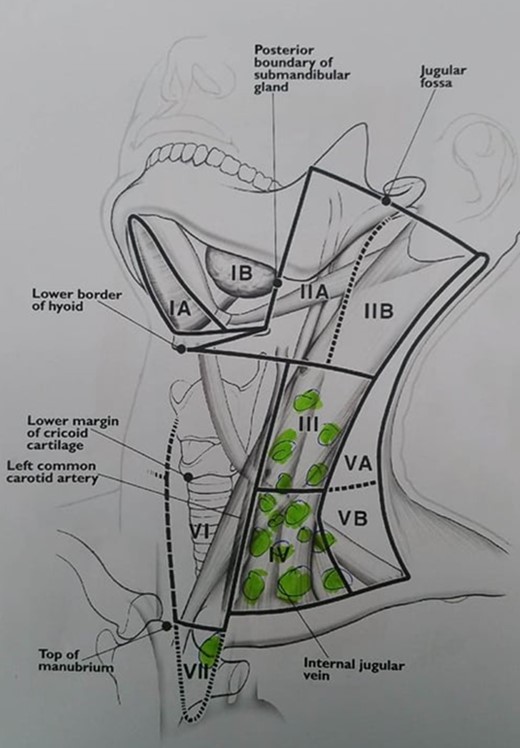
Cervical lymph node mapping.
Under general anesthesia, the patient underwent total thyroidectomy with lymphadenectomy of the left anterior compartment (level VI), as well as the left middle (level III) and lower (level IV) internal jugular chain, as macroscopic infiltration was present (Figs 3 and 4). Level VII lymph nodes were also excised, since one of them was found to be abnormally enlarged and possibly necrotic both on preoperative mapping and during intraoperative inspection. Tracheostomy was not considered mandatory in his condition.
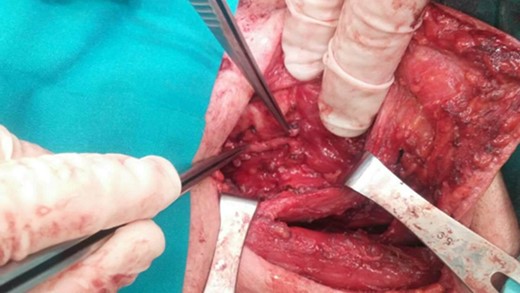
Lymphadenectomy of the left cervical compartments.
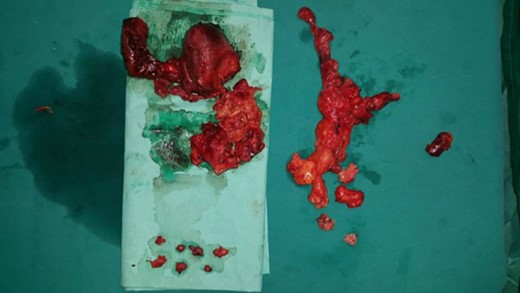
Total thyroidectomy and extended cervical lymphadenectomy. Excised specimen.
The patient did not show operation-induced complications, such as hypoparathyroidism or signs of laryngeal nerve injury, and was discharged in good condition on the first postoperative day.
Pathologic examination of the excised specimen revealed an invasive carcinoma with papillary characteristics in 30% of the specimen and anaplastic characteristics in 70%. Two lymph nodes out of the 6 that were excised from level VII, as well as 22 out of 53 excised from levels III and IV were infiltrated; the overall staging was considered IVB.
Forty-five days after surgery, the patient received adjuvant oral 100 mCi 131I. A total body SPECT scan 6 days after treatment did not show any areas of abnormal distribution (Fig. 5). During the following month, the patient was also administered 30 doses of external beam radiation therapy (EBRT).

Total body SPECT scan performed after adjuvant radioiodine treatment. No abnormal distribution is observed.
On follow-up examinations at 3-month intervals, the patient reported an optimal quality of life with no health issues. CT scans at the same 3-month intervals were performed, which also showed that the patient was completely disease-free, with no signs of recurrence or distant metastases.
DISCUSSION
ATC is usually diagnosed clinically, due to a cervical mass rapidly enlarging over a period of weeks, along with compression symptoms [4]. Extensive local invasion upon time of diagnosis, with lymph node metastases, are present in 60% of the cases [5]; distant metastases may also be already present [6]. Due to its aggressive characteristics and poor prognosis, ATC is classified as a TNM stage IV tumor [2]. Core biopsy is critical in the differential diagnosis of other conditions, such as lymphoma, while cervical imaging can reveal locoregional disease, and further CT imaging or PET-CT can show any distant spread.
Complete resection is hypothesized to improve survival. However, since R0 excision is not feasible in the majority of cases, palliative surgery is commonly performed, in order to control central compartment disease. Radiotherapy, with or without surgery or chemotherapy,can also achieve locoregional control of the disease, and is well tolerated, but does not seem to prolong survival [7]. Currently used chemotherapeutic agents include doxorubicin, either alone or in combination with other agents, in conjunction with radiotherapy [8].
The importance of ultrasound imaging of the cervical lymph nodes has already been proven in cases of thyroid cancer, due to the association of lymph node invasion with locoregional recurrence and decrease of disease-free survival. Preoperative ultrasound can determine the extent of the primary tumor, and subsequent lymph mapping can help to achieve better surgical plans and improved survival, resulting in modifications to the surgical approach in 40% of cases. Specifically, mapping leads to precise cervical lymph node dissection, especially in patients with multiple positive lymph nodes, who present a greater risk of recurrence. Relevant studies in cases of differentiated and medullary thyroid cancer have already revealed the value of lymph mapping in accurate surgical planning and prognosis [9]. However, lymph mapping in cases of anaplastic thyroid cancer has not been described in the current literature, thus indicating the innovation of our treatment.
In our case, lymph node mapping was performed by a specialized radiologist and was crucial in the establishment of the extent of cervical lymph node infiltration, as well as the subsequent lymphadenectomy and achievement of R0 resection. Therefore, preoperative performance of cervical lymph node mapping in cases of ATC could also be useful when deciding the most accurate surgical intervention.
In our case, further adjuvant therapy with radioactive131I and EBRT was performed postoperatively. Triple therapy has actually been shown to yield favorable results in a recent, limited retrospective study [10]. Early diagnosis, prior to the occurrence of distal metastases, also helped in this patient’s favorable results.
As mentioned previously, although the extent of resection remains controversial, total thyroidectomy with extended lymphadenectomy, after timely lymph node mapping, along with multimodal postoperative treatment, demonstrates, in the case examined here, the feasibility of R0 resection and improved survival.
CONFLICT OF INTEREST STATEMENT
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial or non-financial interest in the subject matter or materials discussed in this manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}