





Abstract
In the case where intraoperative endoscopy is necessary and there is no endoscope available in the hospital, there is a solution, the use of available laparoscopic equipment. The technique is simple and without being time consuming. All its needed is a laparoscopic video- camera, and laparoscopic ports. The whole procedure takes place in the surgical field and provides an immediate solution for the endoscopic inspection of stomach, small intestine and large intestine. We describe the first case where it takes place in an open right colectomy in a patient with colon cancer and a suspicious lesion at the left colon. Further studies are needed to evaluate the indications and the effectiveness of the method.
INTRODUCTION
Intraoperative colon endoscopy during colorectal surgery was first published in 1973 by Richter et al. [1]. Since then, this technique has been applied in new cases and for new indications. Colorectal surgery, either laparotomy or laparoscopic/robotic-assisted, allows the surgeon to investigate the outside part of intestinal wall, while colonoscopy allows the imagining of the colon from the inside. The review of Kawai et al. [2] analyzed the benefits of intraoperative colonoscopy.
These are:
Determination of the tumor site,
Observation of the proximal part of the colon,
Anastomosis line checking
CASE REPORT
A 70-year-old female patient, presents with constipation, changes in bowel habits and fecal bleeding. After the workup, she is diagnosed with colorectal cancer. Pre-operative colonoscopy described a large (about 5 cm) tumor after the splenic flexure at 80 cm from anal verge and a suspicious lesion at 40 cm that cannot be identified endoscopically. The tumor at the right colon is described as a blown mass circularly occupying the cavity and blocking the passage of the endoscope. Biopsies were taken and the histopathologic examination revealed moderate and low-grade adenocarcinoma. The patient underwent a CT-scan which described a volumetric thickening of the ascending colon, a 3.4 cm tissue with a density of soft particles and the presence of swollen lateral lymph nodes.
The patient underwent an exploratory laparotomy. A middle abdominal incision is performed. A mass is found in the middle of the anionic colon infiltrating the lateral peritoneal attachment. A right colectomy [part of the terminal ileum, cecum, the ascending colon, the hepatic flexure and the first third of the transverse colon, along with fat and lymph nodes] is performed. Because of the doubt about the existence of synchronous colonic cancer, which was not confirmed optically and tactile, intraoperative colonoscopy is considered necessary.
TECHNIQUE OF INTRAOPERATIVE COLONOSCOPY
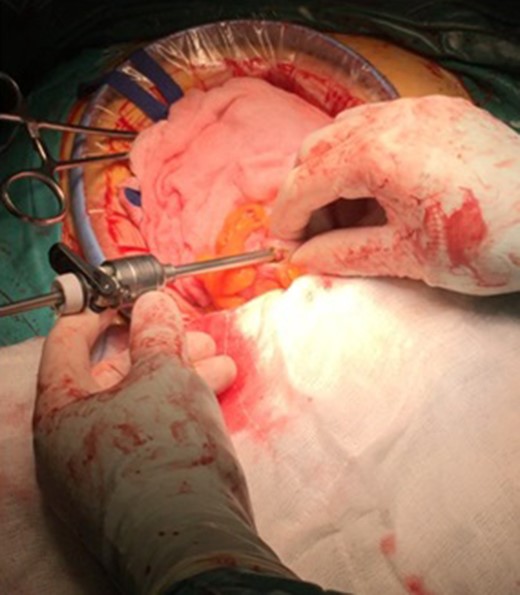
An isolation of the peritoneal cavity with compresses was initially performed. A cross-section of the peripheral truncation was performed on the colonic tape at the point where the ileocolonic anastomosis would be later created. A 10 mm laparoscopic port was inserted in the hole and CO2 insufflations started (Fig. 1). After bowel dilatation the camera was inserted through the laparoscopic port in the colon lumen. During the time the camera is intraluminal, water injection is provided, to avoid thermal injury of the mucosa. Overview of the lumen, until the splenic flexure bend and the beginning of the descending colon was performed. A hole was then applied to the colic tape at the lower third of the sigmoid (Fig. 2). Again, a 10 mm laparoscopic port was inserted and the laparoscopic camera was used to inspect the bowel lumen up to the splenic flexure. After the endoscopic inspection of the bowel has been completed, the laparoscopic ports were withdrawn (Fig. 3). The holes were converged with seromuscular stitches of the sigmoid and omentumplasty. A stapled side to side anastomosis was hen performed between terminal ileum and colon. The patient discharge hospital without any complication on the eighth postoperative day. The histopathology of the specimen shows low grade adenocarcinoma of the colon, pT4bN1b.

The insertion of the port at transverse colon and the isolated operation field with compresses.
The insertion of the port at the sigmoid colon and the isolated operation field with compresses.
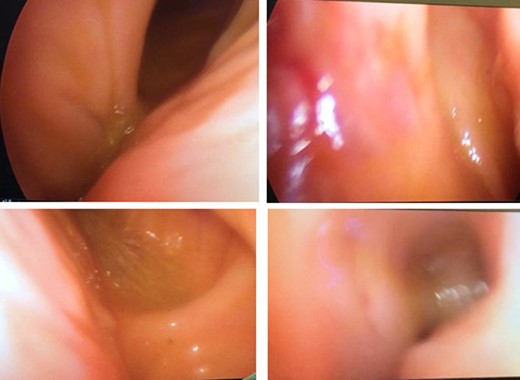
Intraluminal view of the colon through the laparoscopic video camera.
DISCUSSION
Intraoperative colonoscopy is a useful technique that helps confirmation of the integrity of anastomosis [3], while it can identify bleeding from anastomosis, bleeding spot in lower digestive hemorrhage, synchronous neoplasms in the large intestine and a fistula in an inflammatory bowel disease. It can be also used to accurately locate an intestinal lesion and determine the length of colon excision. [4] The described technique gives the surgeon the flexibility to move safely to the next step of his intervention with the advantages of low cost due to multi-purpose materials and no additional surgical manipulations in the surgical field. Pontone, used a similar technique but for the intraoperative enteroscopy, by using a typical colonoscope, through a 15-mm laparoscopic port [5]. This technique did not affect the outcome of the patient nor the morbidity due to possible early complications associated with surgery and endoscopy.
Due to lack of data on the reported technique, it is a challenge to record new incidents and collect data in order to demonstrate its safety and effectiveness in the field of small intestine, colon and stomach surgery, in the absence of a colonoscope or gastroscope, taking also into account the lower time required by this method compared with the use of a colonoscope and gastroscope from the anus and the mouth, respectively.
In this case, the bowel has been prepared preoperatively with antibiotics per oral and intravenous, to limit the risk of an intraoperative infection.
The use of this technique in emergency surgery is also a field of research into its effectiveness. Through a hole in colon wall, the surgeon can have a direct overview of the lumen allowing moving into the next step of the intervention. Naturally, in regular interventions for benign or malignant lesions of the colon in which intraoperative endoscopy is deemed necessary, the described technique can provide a reliable solution.
CONCLUSION
Intraoperative colon endoscopy is a feasible and safe technique when intraoperatively endoscopy is needed. However further studies are needed to evaluate the indications and the effectiveness of the method.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}