





Abstract
The presence of vermiform appendix in an inguinal hernia sac is known as Amyand’s hernia. Amyand’s hernia complicated with acute appendicitis is an extremely rare entity with challenging diagnosis and large debate about the optimal treatment option. We report a case of a 58-year-old man presenting to the Emergency Department with an incarcerated right inguinal hernia. At laparoscopy, an inflamed appendix was identified within the inguinal canal, representing an indirect Amyand’s hernia. A laparoscopic appendicectomy was performed followed by a trans-abdominal pre-peritoneal mesh repair of the aforementioned hernia. We report this rare clinical entity raising physicians’ awareness to include acute appendicitis within an Amyand’s hernia in the differential diagnosis of incarcerated inguinal hernias, along with a successful minimally invasive surgical approach.
INTRODUCTION
Inguinal hernias are one of the most common clinical problems encountered in adults. Amyand’s hernia is defined as a protrusion of the vermiform appendix in an inguinal hernia sac. Amyand’s hernia has a prevalence of 0.5% of all inguinal hernias and is considered a rare clinical entity with a difficult clinical and imaging diagnosis. A large debate exists about the optimal treatment [1]. Herein we report a case of a 58-year-old man with an incarcerated right inguinal hernia that was managed using a laparoscopic trans-abdominal pre-peritoneal (TAPP) approach. Intra-operatively an Amyand’s hernia with acute appendicitis was identified. We describe this rare clinical entity along with a successful surgical approach.
CASE REPORT
We report a rare case of a 58-year-old male, presenting to the Emergency Department with worsening vague right lower quadrant abdominal pain and vomiting for the past 48 hours. His past medical history was unremarkable. Clinical examination revealed an irreducible and tender right inguinal hernia, with mild tenderness at the right lower quadrant on deep palpation. Full blood count revealed leukocytosis (15.300 per mm3) with right shift. The rest of the clinical and laboratory test were normal.
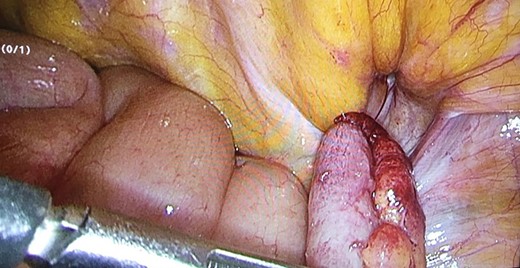
As a result, the patient was admitted to our surgical ward and scheduled for an emergency surgical repair of the incarcerated right inguinal hernia. A trans-abdominal laparoscopic approach to repair the hernia and at the same time to inspect the hernia contents was utilized. A 10 mm camera port was placed subumbilically and a further 5 mm and 10 mm working ports were placed under direct vision at the lower midline and right iliac fossa respectively. Laparoscopy revealed the presence of an indirect right inguinal hernia containing the appendix (Fig. 1). Reversing the content of the hernia revealed an inflamed appendix at its distal half (Figs 1 and 2). Laparoscopic appendicectomy for acute appendicitis was performed, followed by a TAPP mesh repair of the right inguinal (Figs 3 and 4). Operative time was 55 mins and estimated blood loss was 50mls. One dose of penicillin-based antibiotic was given at induction, followed by two further doses eight hourly. The post-operative course was uneventful with patient discharged the following day.

Sliding indirect right inguinal hernia during laparoscopy with vermiform appendix as content of the sac (Amyand’s hernia).
Inflamed vermiform appendix as content of the sac.

Hernia’s orifice after reversal of the sac’s content.

Laparocopic mesh placement.
Histopathological assessment of the vermiform appendix confirmed the diagnosis of acute appendicitis with neutrophilic infiltrates of the appendiceal wall and acute mucosal inflammation.
DISCUSSION
Amyand’s hernia was first described by Claudius Amyand in 1735 [2]. It can occur at any age, mostly in men and is three times more common in children than in adults [3, 4]. The pathophysiology of this rare condition is unknown, but the most common explanation is that the vermiform appendix herniates through a patent processus vaginalis. The hernia sac and the testis may sometimes connect through a fibrous band that attracts the appendix [1].
Vermiform appendix may remain in the hernia sac without causing symptoms throughout the patient’s life or the neck of the hernia can strangle it causing vascular obstruction, inflammation (appendicitis), perforation and peritonitis [1]. Acute appendicitis, as in this case, is reported in only 0.08-0.013% of cases and usually clinical presentation of Amyand’s hernia mimics that of an incarcerated inguinal hernia [2]. Majority of patients present to the emergency department with non-specific signs or symptoms, thus making the clinical diagnosis challenging, if not impossible [4].
Pre-operative diagnosis of Amyand’s hernia through imaging is extremely difficult, but feasible with ultrasound and CT scans. Pre-operative information on the appendix may not even be useful as regards to treatment decisions. Ultrasound may reveal a blind-ended tubular structure with thickened wall inside the hernia sac. CT may set the diagnosis of Amyand’s hernia through direct visualization of the appendix inside the inguinal canal or location of the cecum in proximity to the hernia sac [1–3]. In our case pre-operative ultrasound or CT scans were not performed and the patient was consented for emergency diagnostic laparoscopy with simultaneous hernia repair[2, 3]. this is not uncommon practice as most painful groin lumps end up in the operating room for exploration and hernia repair without prior imaging (Kromka’s et al. and Abdulla’s et al.)
Α large debate exists regarding the optimal treatment of Amyand’s hernia and whether prophylactic appendicectomy and mesh repair are essential. Classical treatment includes reduction of hernia, appendicectomy and hernioplasty. When the appendix is found inflamed, then appendectomy is recommended; when the appendix is uninflamed, some support appendectomy due to high risk of reherniation or future appendicitis, while others claim that appendectomy increases the operative risk and thus do not support it [1–3]. In regards to mesh placement, some surgeons propose avoidance of its use in the presence of appendicitis due to a higher risk of septic complications like wound infection, systemic sepsis and fistula formation. On the contrary, others report no septic complications with mesh placement in inflamed cases and are so supportive of its use. Nowadays, minimally invasive techniques have gained ground in the management of hernia repair and are used worldwide with increased frequency. As a result, a few cases of Amyand hernias have been reported in the literature as being managed with a minimally invasive approach. The first laparoscopic repair without a mesh in an Amyand hernia was performed in 1999, while the first laparoscopic repair with mesh placement was performed in 2004 [1]. When performing laparoscopic TEP (total extraperitoneal) hernioplasty, Amyand’s hernia may not be recognized, as intraperitoneal structures are not typically inspected and a case of acute appendicitis may be missed with perplexing consequences postoperatively. Abdulla et al. suggested an open repair of the inguinal hernia without a mesh along with laparoscopic appendicectomy, while Sahu et al. reported laparoscopic TAPP repair with mesh without appendicectomy in three patients treated for elective inguinal hernia. In our patient, we decided to perform laparoscopic TAPP repair with mesh placement along with laparoscopic appendicectomy, despite the fact that the vermiform appendix seemed inflamed, without facing any complications postoperatively.
In conclusion Amyand’s hernia is a rare entity especially when combined with acute appendicitis. Hence, we suggest that this particular condition should be considered in the differential diagnosis of patients with incarcerated inguinal hernia. Minimally-invasive techniques such as laparoscopic hernia repair with mesh placement and appendicectomy may be a feasible, safe and effective method in the management of complicated Amyand’s hernia.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}