





Abstract
Since the therapeutic use of cannabis and its derivatives is currently rising, the adverse effects of cannabis and cannabinoids are of special interest. However little is known about the possible effects of long-term use of cannabis on the gastrointestinal motility. Herewith we describe the case of a patient with a rare severe form of intestinal intussusception following long-term cannabis consumption. The case shall raise awareness of possible life threatening complications of the use of cannabis and its derivates.
INTRODUCTION
We present the rare case of severe form of intestinal intussusception in an adult patient with cannabis abuse. We propose, that in patients with known chronic use of cannabis or cannabinoids and abdominal pain, a special attention should be paid to the disease with impaired gastrointestinal mobility like previously described delayed gastric emptying [1] or spontaneous intussusceptions. The objective of this case report is to increase the awareness of healthcare professionals to the adverse effects of cannabinoids on gastrointestinal motility.
CASE REPORT
We present the case of a 30-year-old male patient who was admitted to our emergency department with a 24 h history of severe abdominal pain, diarrhea and vomiting. During clinical examination, the patient reported mentioned an episode with identical symptoms three months before that was treated conservatively at another institution. The patient’s past medical history included posttraumatic stress disorder and chronic consumption of cannabis via inhalation (10–15 joints a day). The pain intensity was so strong that the patient was observed by his girl-friend to sluice boiling water on his body. In the hospital at admission the patient was aggressive and endangered himself and others. The blood test demonstrated an increased leucocyte count with 16.88 G/l, but a normal C-reactive protein level with 0.1 mg/dl. At first, the patient was treated with lorazepame and olanzapine under clinical suspicion of acute psychosis related to his cannabis consumption. Due to further exacerbation of the pain, a CT scan was performed showing several small bowel intussusceptions in the left abdominal region (Fig. 1A and 1B). Because of the acute abdominal symptoms and the findings in the CT scan a diagnostic laparoscopy was performed. Intraoperatively numerous, at least ten, regions of jejuno-jejunal intussusceptions were found (Fig. 2A, Video 1). The intussuscepted jejunal segments were repositions by careful stretching of the small bowel. During examination of the affected bowel segments there was no evidence of a tumorous lesions or any other pathology (Fig. 2B). Only the intestinal content appeared thickened and pasty. Most interestingly severe atony of the whole small bowel was observed (Fig. 2A, Video 1). Because no ischemic leasions or other pathology was found, no intestinal resections deemed necessary and the operation was terminated. The patient developed no surgical complications, and had bowel movements after gastrografin application. Due to a good recovery, he was discharged on postoperative Day 2 with recommendation of adequate liquid intake and use of laxatives on demand.
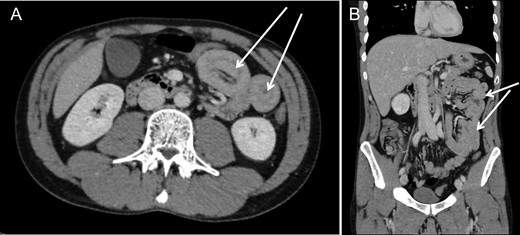
Computed tomography revealed presence of several jejuno-jejunal intussusceptions in axial (A) and coronar (B) images.
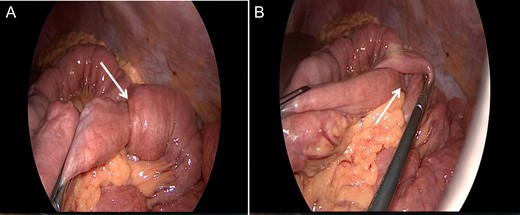
Diagnostic laparoscopy showing multiple intussusceptions (arrow) without any further pathologic findings.
DISCUSSION
Acute intussusception with complete intestinal obstruction is one of the main reasons for ileus formation in children [2]. Presentation of adult patients with acute intestinal intussusception is rare, accounting for only 5% of all cases of intestinal obstructions, and about 86–90% of them demonstrate organic reasons [3–5]. In a retrospective study with 41 adult patients with postoperative diagnosis of intussusception, 54.5% of the intussusceptions were caused by a tumor, of which 27.3% were malignant, and 9.1% comprised non-tumorous polyps, and only four (9.8%) intussusceptions revealed no organic lesion [4].
Cannabis and cannabinoids are the most widely available and used drug across the world [6]. The receptor system for main active ingredient of cannabis, tetrahydrocannabinol, consists of two receptors, the cannabinoid type 1 receptor (CB1) and the cannabinoid type 2 receptor (CB2). CB1 receptors are located throughout the gastrointestinal tract, predominantly in myenteric and submucosal neurons, as well as non-neuronal cells such as epithelial cells (reviewed in [7]). CB2 receptors are mainly located on inflammatory and epithelial cells. It was demonstrated for cannabis and cannabinoids that interaction through inhibition of intrinsic cholinergic mechanisms can result in inhibition of gastrointestinal motility (reviewed in [7]).
Since the therapeutic use of cannabis and its derivatives is currently increasing, additional attention should be paid to the adverse effects of cannabis and cannabinoids. The known possible effects of long-term use of cannabis and cannabinoids include addiction, altered brain development, poor educational outcome, cognitive impairment, chronic bronchitis, increased risk of chronic psychosis disorders [6, 8]. There are only single reports that intussusception is possibly associated with chronic inhaled cannabis use [8, 9].
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
The first author was supported by a Clinical Leave Stipend from the German Center of Infection Research ((DZIF) (grant TI07.001; http://www.dzif.de).
REFERENCES

{kind=link}
{kind=link}