





Abstract
The urachus is an embryonic tube that connects the upper portion of the bladder to the umbilicus, and obliterates normally during embryonic development stages forming the median umbilical ligament. Incomplete obliteration of this tube results in many anomalies such as congenital patent urachus, umbilical urachal sinus, vesicourachal diverticulum and urachal cyst. We report in this case a 5-year-old female presented to the Emergency, complaining of generalized abdominal pain, fever, vomiting, and constipation with no umbilical discharge. The clinical presentation accompanied by radiology investigations suggested a case of acute abdomen. We performed an exploratory laparotomy and found a mass above the bladder connected to the umbilicus; we excised the mass and sent a specimen to pathology that confirmed Urachal cyst. Urachal cyst is usually asymptomatic unless it is complicated; depending on our case, we recommend surgical management by complete excision for complicated urachal cyst.
INTRODUCTION
The urachus is a fibrous tube formed by remnants of the allantois and obliterates gradually during normal embryonic development.
Abnormal obliteration results in many anomalies including urachal fistula, diverticulum, sinus and urachal cyst, which is the most common variety [1].
Urachal cyst is a rare condition, commonly seen in children and rarely in adults, usually it stays silent clinically, but complications are possible where acute abdomen symptoms are seen and surgical intervention is indicated.
In most cases, Urachal cyst is asymptomatic, unless it is complicated, such as an infected cyst, calculi formation, or malignancy development.
In our case, we report an infected urachal cyst in a 5 year-old female presented with acute generalized abdominal pain, fever, vomiting, and constipation and managed by surgical excision.
CASE PRESENTATION
A 5-year-old Caucasian female presented to the emergency room complaining of generalized abdominal pain that had started 18 hours prior to presentation accompanied with fever (39 ˚C), vomiting and constipation.
Her past medical history was unremarkable.
On physical examination, she was febrile, the abdomen was rigid and there was generalized severe tenderness.
Digital rectal examination (DRE) showed soft stool without any blood.
Her chest was clear.
Laboratory tests were normal including Hemoglobin (Hb), White Blood Cells (WBC), Platelets (PLT), prothrombin time (PT), INR, Glucose, Creatinine, Urea, Na+, and K+.
C - reactive protein (CRP) was elevated (134.5 mg/l).
Through investigations, erect Abdominal X-RAY (AXR) showed air-fluid levels in the small bowel and dilated loops of the large bowel (Fig. 1).

Erect AXR showing Air-Fluid levels and distended large bowel loops.
Abdominal ultrasonography revealed a 5-cm hyperechoic mass in the hypogastric region surrounded by intestines (Fig. 2).

Abdominal Ultrasonography showing a 5-cm hyperechoic mass above the bladder and surrounded by intestinal loops.
Non-contrast abdominal computed tomography (non-contrast CT) demonstrated a high-density midline mass above the bladder (Fig. 3).
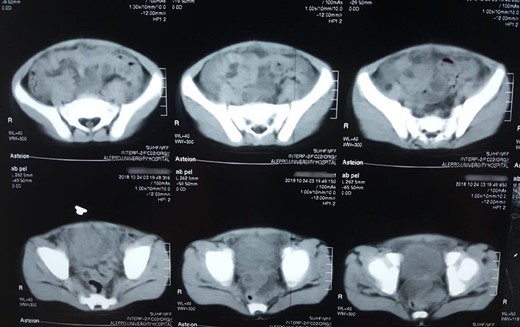
Abdominal non-contrast CT scan showed hyperdensity mass above the bladder.
These findings combined with clinical presentation suggest a case of bowel obstruction that turned out to acute abdomen pain. Therefore, we performed an exploratory laparotomy, and found a 5-cm cystic mass above the bladder, connected to the umbilicus with a purulent productive orifice (Fig. 4), there was purulent fluid between the intestinal loops (approximately 50 ml), and bowel loops were distended.

Intraoperative view of the cyst with a purulent orifice.
We performed complete excision of the mass.
Methylene Blue Dye Injection in the bladder revealed no connection or fistula between the bladder and the mass.
Pathology report of the excised specimen was compatible with Remnant of Urachus with acute suppurative inflammation, and no evidence of malignancy was noticed (Fig. 5).
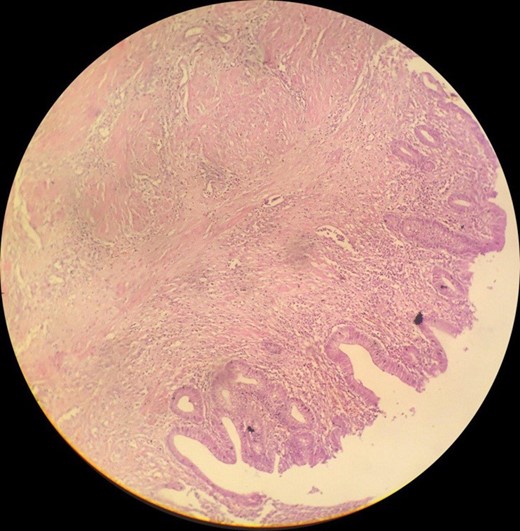
The mass cavity is lined by intestinal epithelium filled with purulent exudate infiltrating the wall that contains muscular layer.
After surgery, the patient had a good condition and started oral nutrition on the next day.
DISCUSSION
Embryologically, the urachus is a tubular structure that connects the dome of the developing bladder to the allantois at the level of the umbilicus. The lumen usually obliterates and eventually becomes a fibrous cord. Incomplete obliteration of the urachal lumen results in one of the five following anomalies: congenital patent urachus; umbilical urachal sinus; vesicourachal diverticulum; urachal cyst; and alternating sinus [1, 2].
The most frequent form of urachal anomalies is the urachal cyst at rates of 30% and it is more frequent in males. Unless complicated, the urachal cysts are usually small, silent and asymptomatic. Complications may include infection, bleeding within the cyst, enlargement, intraperitoneal rupture, intestinal fistula, intestinal obstruction, lithiasis, and a high incidence of malignant degeneration. In the differential diagnosis, vitelline duct anomalies, appendicitis, granulomatous inflammations, and granulation tissue from the umbilical stump should be kept in mind [3].
In our patient, the cyst was located in the hypogastric area and was surrounded by fixed intestinal loops. Patients with infected urachal cysts can present with a wide range of symptoms. The most common symptom of presentation is abdominal pain, which was the case in our patient. Diagnosis is often made following exploratory laparotomy for an unexplained acute abdomen. Complications of infection include sepsis, fistula formation and rupture leading to peritonitis [4].
In our case, rupture of the cyst caused peritonitis.
Radiologic evaluation of urachal cyst by USS, CT and/or MRI is essential for confirming diagnosis.
Ultrasound scan (USS) can help to make diagnosis in 77% of patients. [5]
In our case, the USS was not specific and CT scan was used to help make the diagnosis.
Ultimately, the treatment of choice is complete excision, and open excision is the approach of choice. Open excision was applied to our patient and the excised cyst was sent to pathology, which confirmed it was Remnant of Urachus accompanied by suppurative inflammation.
Complete excision is important because malignant degeneration of the remnant is possible [6].
In cases where preoperative diagnosis has been made, a staged approach with antibiotics followed by surgery has been recommended [4–7].
CONCLUSION
Infected urachal cyst should be kept in mind as a differential diagnosis when approaching an acute abdomen patient, due to its dangerous complications, which in some cases can be fatal. However, it can be completely avoided if it was early diagnosed and properly treated. Ultimately, complete surgical excision remains as the most-preferred approach of treatment, especially when taking in mind the urachal cyst malignant potency.
CONFLICT OF INTEREST STATEMENT
We have no Conflict of Interest.
FUNDING
There are no funding sources.
AUTHOR’S CONTRIBUTION
Conception and design: AKD, AST, ON
Analysis and interpretation of the data: AA, AA, AKD
Drafting of the article: AA, AST, AA, ON
Critical revision of the article for important intellectual content: KA, AKD
All authors read and approved the final version of the manuscript.
CONSENT FOR PUBLICATION
An informed consent was signed by the patient.
REFERENCES

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}