





Abstract
Locally advanced urothelial carcinoma of the renal collecting system presents a unique challenge to the urologist performing nephroureterectomy, particularly if the tumor invades the renal vein or the IVC. Preoperative planning and a multidisciplinary approach are important to optimize the outcomes for these patients. The use of robotic assistance for laparoscopic nephroureterectomy has become common, but a simultaneous robotic assisted IVC excision has yet to be reported. This case report describes a robotic assisted laparoscopic right nephroureterectomy with IVC resection and retroperitoneal lymphadenectomy for locally advanced urothelial carcinoma. For a patient with locally advanced urothelial carcinoma of the renal collecting system which obliterates the renal vein, robotic assisted surgery provides a minimally invasive alternative to open surgery.
INTRODUCTION
About 5–10% of urothelial carcinoma occurs in the upper tract as opposed to the bladder, with an incidence of about 1 per 100,000 person-years in the US [1]. Upper tract urothelial carcinoma occurs most commonly in the pyelocaliceal system (59%) as compared with the ureter (41%) [1]. Nephroureterectomy is the standard of care for large infiltrative upper tract urothelial carcinoma. Of those who undergo nephroureterectomy, pathologic stage T4 disease is only found in 4.9% and lymph node metastasis occurs in 9.9% [2]. The incidence of renal vein or IVC thrombus with urothelial carcinoma is unknown but it is an unusual finding. To the best of our knowledge, this is the first report of robot-assisted laparoscopic nephroureterectomy with IVC excision to address a pT4 urothelial carcinoma.
CASE REPORT
A 51-year-old white male with BMI of 29.7 was referred for gross hematuria. Renal ultrasound identified right hydronephrosis and ureteroscopy demonstrated high grade T2 urothelial carcinoma. CT and MR imaging revealed an 8 cm upper pole infiltrative tumor which obliterated the right renal vein without caval thrombus (Figs 1 and 2). There was no evidence of metastasis on CT chest. The preoperative estimated glomerular filtration rate was 71 ml/min/1.73 m2. Multidisciplinary review was undertaken and a radical nephroureterectomy and lymph node excision was recommended without neoadjuvant chemotherapy.
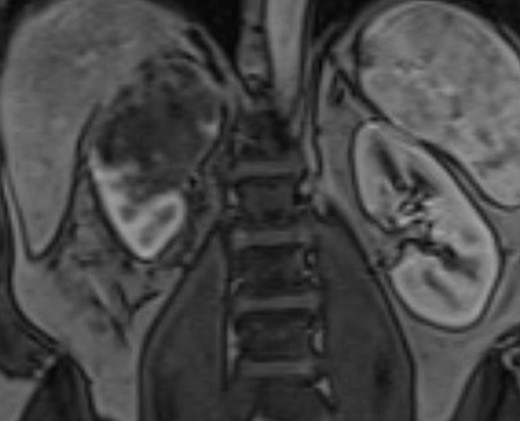
Coronal MRI of the abdomen/pelvis demonstrating the 8 cm right upper pole renal mass.
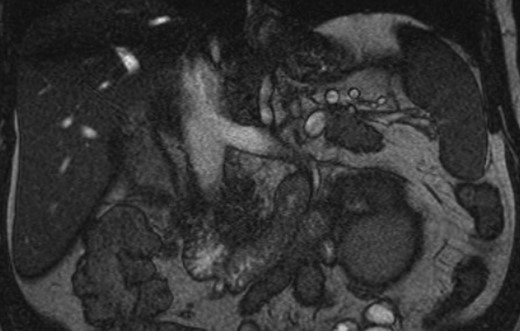
Coronal MRI of the abdomen/pelvis demonstrating no evidence of caval thrombus. The right renal vein was not visible on MRI.
The procedure was started in lithotomy position. The right ureteric orifice was fulgurated with electrocautery and then circumscribed with the Collins knife. The ureter was then ligated inside the bladder with 0-0 Vicryl Endoloop (Ethicon, Somerville, NJ) passed alongside the cystoscope. A 20-Fr catheter was then placed into the bladder.
The patient was repositioned in right flank position. The da Vinci Surgical System Si (Intuitive Surgical, Sunnyvale, CA) was used for the operation. A three-arm robotic approach was used (12 mm camera port located 5 cm lateral to the umbilicus; 8 mm port in the epigastrium for robotic arm #1; 8 mm port in the right lateral mid abdomen for robotic arm #2; and a 12 mm port inferior and medial to the camera port for the assistant). An additional epigastric 5 mm port was used for liver retraction. Consistent with preoperative imaging, the right renal vein was completely obliterated by the tumor, and henceforth, circumferential control of the renal vein was not possible. To accomplish a negative surgical margin, the IVC would need to be partially excised to release the tumor and the right renal vein en bloc.
To accomplish IVC control, the right adrenal vein was ligated and divided. Next, the right gonadal vein was ligated and divided. The IVC superior and inferior to the kidney was circumferentially dissected along with the left renal vein. Rummel tourniquets were used at the suprarenal IVC, the infrarenal IVC, and the left renal vein. No lumbar veins were encountered. The Rummel tourniquets were made from blue silicone vessel loops (Purple Surgical, Shenley, England) doubly wrapped around the vessels and passed through a 1-inch piece of snugger tube (Henleys Medical, Welwyn Garden City, England). The right renal artery was ligated at the interaortocaval location. Prior to IVC clamping, communication with the anaesthesiologist occurred and 5 000 IU of heparin were given intravenously. The three Rummel tourniquets were tightened and secured with 10 mm Weck Hem-o-lock clips (Teleflex Medical, Wayne, PA) – inferior IVC first, left renal vein second, and superior IVC last. The IVC was then incised just medial to the obliterated right renal vein. The Rummel tourniquet at the infrarenal IVC was not completely hemostatic despite additional tightening, and thus the assistant provided pressure with a suction irrigator and a mini-laparotomy sponge to the infrarenal IVC to achieve complete hemostasis. The anterior and posterior walls of the IVC were incised with the robotic scissors, releasing the right renal vein. The IVC was closed with 4-0 polypropylene in running fashion. Prior to completely closing the defect, some blood was allowed through the infrarenal IVC Rummel to allow air to escape from the IVC. The total tourniquet time was 50 minutes. Next, the right kidney was mobilized en bloc with the regional lymph nodes from the vena cava and the interaorto-caval space.
To dissect the distal ureter, the robot was re-docked. The ureter was mobilized to the bladder cuff, confirmed by visualization of the Endoloop on the distal ureter. The ureter was swollen with urine, confirming of the efficacy of Endoloop ligation. The estimated blood loss was 700 ml.
The patient was discharged home on postoperative day three. Cystogram at 14 days postoperatively showed no extravasation and the catheter was removed. At six weeks postoperatively, his estimated glomerular filtration rate was 69 ml/min/1.73 m2, a decrease of only 2 ml/min/1.73 m2. The patient was referred for adjuvant chemotherapy.
The pathology revealed an 8.5 cm tumor that penetrated the renal capsule, but the surgical margin was negative. Microscopy demonstrated a focally necrotic, high-grade (grade 3) urothelial carcinoma that was pleomorphic and showed diffuse permeation of the renal parenchyma. It extended beyond the renal capsule into perinephric fat where it was approximately 1–2.5 mm from the adjacent perinephric fat resection line (pT4). There was widespread lymphovascular invasion. The carcinoma invaded the renal hilar fat, where it encased the main renal artery and extended into perineural spaces and vessels. Two reactive lymph nodes were detected in the hilar fat with one of them containing metastatic carcinoma (N1). Renal vein could not be identified by the pathologist.
DISCUSSION
The development of laparoscopic techniques for addressing IVC thrombus with renal cell carcinoma can be applied to locally advanced upper tract urothelial carcinoma. Fortunately, invasion of the IVC by upper tract urothelial carcinoma is rare and the majority of IVC thrombectomy will continue to be performed for renal cell carcinoma. For urologists who perform robotic nephroureterectomy, familiarization with the techniques of robotic IVC thrombectomy may prove crucial [3, 4].
CONFLICT OF INTEREST STATEMENT
None declared.
DISCLOSURES
Opinions, interpretations, conclusions, and recommendations are those of the author and are not necessarily endorsed by the United States Air Force.

{kind=link}
{kind=link}