





Abstract
We present a case of a 75-year-old male who was referred to an Emergency Department with possible diverticulitis. On further review of CT imaging, extensive sigmoid diverticulosis with mural thickening and inflammatory stranding was noted, with a linear dense foreign body present within the sigmoid lumen. The patient was managed with intravenous antibiotics and colonoscopic retrieval of the foreign body, which was lodged within a diverticulum. This case emphasizes the importance of early colonoscopic management of patients suspected to have a colonic foreign body. We then review the literature regarding colonic foreign bodies and the association with diverticulosis.
INTRODUCTION
Colonic foreign bodies are not an uncommon emergency surgical presentation. However, few reports in the literature explore the association of colonic foreign bodies with diverticulosis. We present a case of a gentleman with an impacted foreign body within a sigmoid diverticulum, mimicking diverticulitis.
CASE REPORT
A 75-year-old male was referred to the Emergency Department from his GP, with possible diverticulitis. He had been unwell for the past 2 weeks, with intermittent lower abdominal pain. There was no associated nausea or change in bowel habit. He denied any recent ingestion of meat or fish bone. His medical history was significant for hypertension, cardiomyopathy and rheumatoid arthritis. His regular medications included clopidogrel. His last colonoscopy was performed 10 years ago for surveillance which was unremarkable.
On examination, the patient was haemodynamically normal and afebrile. He had a soft non-peritonitic abdomen, which was mildly tender in the lower abdomen. Rectal examination was normal. His bloods on admission demonstrated an elevated white cell count 13.2 × 109/l (reference range 3.9–11.1), with rest of the blood work unremarkable.
The patient had an outpatient intravenous contrast-enhanced CT abdomen and pelvis (Fig. 1) which demonstrated extensive sigmoid diverticulosis, with diffuse mural thickening and surrounding inflammatory stranding. The surrounding inflammatory changes extended towards a loop of adjacent small bowel. Within the sigmoid lumen at the site of these changes, was noted to be a linear dense foreign body.
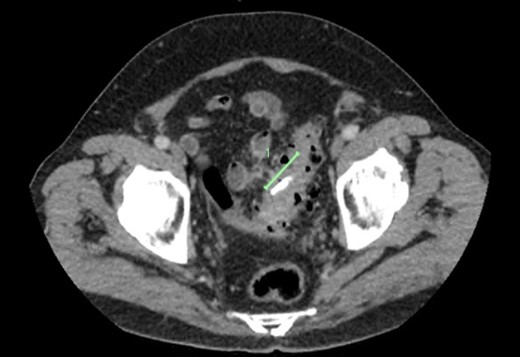
CT demonstrating a radio-opaque foreign body (marked) in segment of sigmoid diverticulosis, with stranding extending to adjacent loop of small bowel.
The patient was admitted to hospital and commenced on intravenous antibiotics. The following day he underwent a flexible sigmoidoscopy, which demonstrated multiple small and large diverticulum in the sigmoid colon. A foreign body was found in the sigmoid colon at 28 cm from the anal verge, suggestive of ingested bone (Fig. 2). The foreign body appeared to be lodged within a diverticulum. Adjacent to this, was a localized area of moderately inflamed mucosa, possibly reactive to the foreign body. No obvious entero-colonic fistula was identified. Biopsies were taken of this inflamed area, which later demonstrated on histopathology to be consistent with non-specific reactive changes. The foreign body was retrieved successfully endoscopically using tripod forceps (Fig. 3).

Colonoscopic view of foreign object within segment of sigmoid diverticulosis.

Foreign object, post-colonoscopic extraction.
The patient recovered well post-operatively and was commenced on a regular diet. He continued on intravenous antibiotic therapy until his discharge from hospital on Day 2 post-procedure.
DISCUSSION
Colonic diverticulosis is a common benign condition, present in over 60% people over 60 years of age [1]. The majority of patients with ingested foreign bodies are asymptomatic, with the foreign object passing without significant event [2]. However, colonic foreign bodies have been associated with diverticulitis, although are a rare cause. Limited cases have been reported in the literature.
It has been theorized that the structural changes associated with diverticulosis, such as a ‘potentially tortuous lumen, strictures and mural pockets’ [3], may make it a potential environment for foreign bodies to lodge. Typically, the ingested foreign bodies are food-related items, such as chicken or fish bones; phytobezoars have even been described. Several cases of toothpick impaction in diverticulosis have also been associated with foreign body impaction in diverticulosis.
Patients may present with signs typical for acute diverticulitis; with left iliac fossa pain and tenderness, and elevated inflammatory markers [4, 5]. In more advanced cases, patients may also present with colonic perforation, colo-vesical fistula, peri-colic abscess, entero-colonic fistula, and even colo-arterial fistula have been described [3].
CT is the imaging modality of choice for diagnosis (as in the case of our patient), however the diagnosis of a foreign body may not be identified until time of colonoscopy or even laparotomy.
Management is dependent upon both patient related and pathology related factors. The majority of colonic foreign bodies will pass without intervention. In patients with impacted foreign bodies associated with diverticulosis, who are clinically well without evidence of perforation, colonoscopic removal of the foreign body may be safely achieved, as in this patient’s case. In unwell patients with features of perforation, laparotomy and colonic resection may be performed. Laparoscopy and washout of a localized foreign body caecal diverticular perforation has also been described [6].
ACKNOWLEDGEMENTS
Thank you to Dubbo Base Hospital theatre staff for their assistance with this case.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}