





Abstract
The presence of the gallbladder in a parastomal hernia is exceeding rare. We present the case of a 75-year-old female with a parastomal hernia complicated by presence of the gallbladder. The patient was managed with surgical intervention to repair the hernia and reduce the gallbladder to its correct abdominal position without cholecystectomy. She recovered well from her surgical repair, and was recurrence free at her 6-month outpatient visit. This is the one of seven reported cases of parastomal gallbladder herniation and fits with known pre determinants of advanced age and being female. We present this case due its interesting and novel nature.
INTRODUCTION
We present the case of a 75-year-old lady with gallbladder parasotmal herniation in which hernia repair was performed without cholecystectomy.
CASE REPORT
Ms JM, a 75-year-old female presented to a tertiary hospital emergency department with colicky right upper quadrant abdominal pain that had increased in severity and frequency over a week. This was associated with pain radiating to the back, as well as intermittent nausea and vomiting.
She had previously undergone open subtotal colectomy and formation of end ileostomy for sigmoid volvulus two decades ago. This was complicated by recurrent parastomal hernias requiring surgical repairs which included local repair with mesh, repositioning of the stoma to left upper quadrant then finally to the right upper quadrant. She had a BMI of 31.2 kg/m2.
On clinical examination, there was evidence of a large irreducible parastomal hernia associated with the end ileostomy in the right upper quadrant. Contained within the parastomal hernia, there was a firm palpable mass. The stoma appeared healthy and was reported to be functioning well.
Subsequent Computed Tomography (CT) of the abdomen and pelvis revealed a parastomal hernia containing the gallbladder (Figs 1 and 2). There was no evidence of cholecysitis or choledocholithiasis. CBD was dilated to 9 mm without any filling defects.
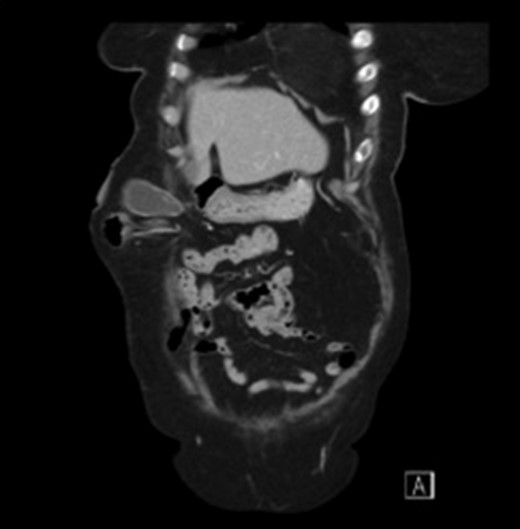
Sagittal view CT scan of the gallbladder in the parastomal hernia.
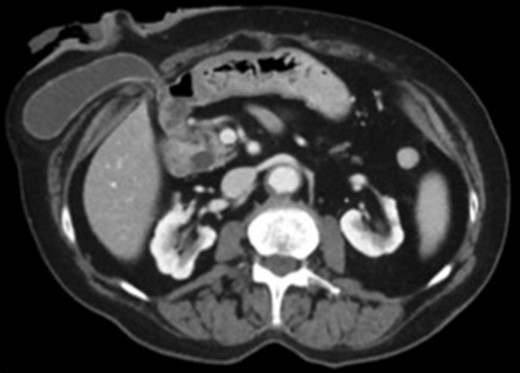
Axial view CT scan of the gallbladder in the parastomal hernia.
Surgical management was decided after discussion with the patient. Intra-operatively, a transverse incision lateral to the stoma was performed. The Hernia sac was identified and its contents were inspected. Among small bowel loops, the gallbladder was present within the hernia sac. The Gallbladder was not inflamed or ischaemic and was easily reduced into the peritoneal cavity. No cholecystectomy was performed.
The parastomal hernia neck was tightened and onlay mesh (ULTRAPRO® Ethicon, USA) was used to reinforce the parastomal hernia site.
She recovered well post-operatively without immediate complications and was discharged home 4 days after the operation with oral analgesia. At her 6-month outpatient clinic review, no recurrence of parastomal hernia was noted.
DISCUSSION
Presence of the gallbladder in a parastomal hernia is exceedingly rare. According to the literature, there are only seven other reported cases. There is a predominance for the elderly, with the average patient age of these seven cases being 75.4 years of age and all but two cases being female [1–7]. Suggested factors for occurrence in the elderly are elastic tissue, reduced intra-abdominal fat, liver shrinkage and increased gallbladder mesentery [8].
Of the prior reported gasses of gallbladder herniation, there has been a mix of management routes. In the absence of signs of cholecystitis, the gallbladder had not been removed, one being manually reduced without surgery and one being reduced intraoperatively. In the majority of cases, the gallbladder was incarcerated or showed signs of cholecystitis within in the hernia, requiring emergent intervention with cholecystectomy. In those patients with signs of cholecystitis who had significant co-morbidities or refused further surgery, conservative management was undertaken [1–7]. See Fig. 3 for summary of management routes (cholecystectomy vs no cholecystectomy).
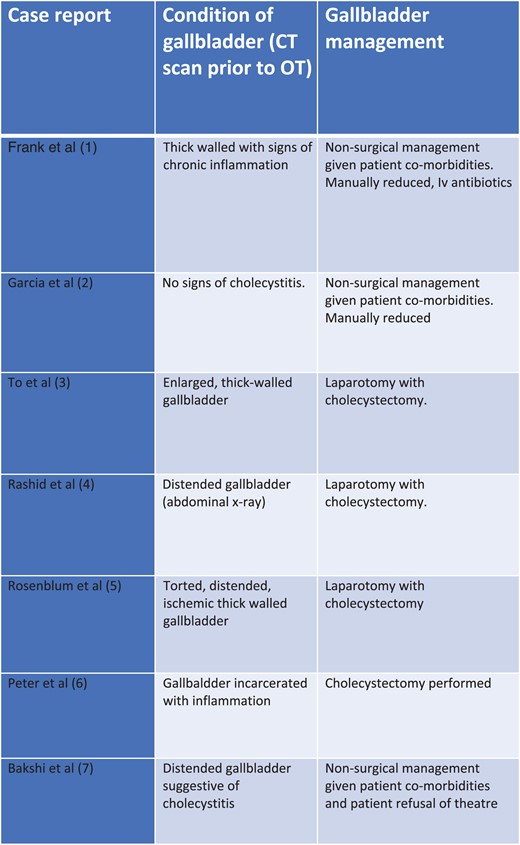
Management routes for gallbladder parastomal herniation (cholecystectomy vs no cholecystectomy).
In the case we present, there were no signs of acute cholecystitis or incarceration, therefore the gallbladder was reduced intra-operatively without cholecystectomy. Given the mesh repair, cholecystectomy would have increased the risk of mesh infection.
In conclusion, we present the case of a 75-year-old female with a parastomal hernia complicated by presence of the gallbladder. The patient was managed with surgical intervention to repair the hernia and reduce the gallbladder to its correct abdominal position without cholecystectomy. She recovered well from her surgical repair, and was recurrence free at her 6-month outpatient visit. This is one of the seven reported cases of parastomal gallbladder herniation and fits with known pre determinants of advanced age and being female. Based on these prior reports, the operative decision appears to be determined by the condition of the gallbladder (cholecysitis or not) and the patient co-morbidities. We present this case due its interesting and novel nature.
CONFLICT OF INTEREST STATEMENT
None declared.
DECLARATION
The corresponding author has received no research scholarship. This submission has not been concurrently communicated with any other journal or association

{kind=link}
{kind=link}
{kind=link}