





Abstract
Bowel perforation due to inadvertent ingestion of foreign objects is, fortunately, a rare event. However, it can lead to deadly complications when it occurs. Thin, sharp and pointed objects like toothpicks are more likely to pierce the bowel wall. Diagnosing toothpick ingestion and perforation is difficult since most patients do not recall swallowing the toothpick, symptoms and physical examinations are nonspecific, the symptoms can resemble many abdominal pathologies, and since a toothpick has a radiolucent nature that makes it difficult to detect through X-ray imaging. Due to this, most of the cases are identified during the transoperative period. We present the case of a 27-year-old male who presented with symptoms clinically indistinguishable from acute appendicitis. During surgery, two toothpicks were discovered that compromised the cecum and the appendix. After successful removal of the foreign objects, the patient underwent a full recovery.
INTRODUCTION
Ingestion of foreign bodies is a common event observed on clinical practice. However, only a limited number of patients remember the incident, making diagnosis challenging for the clinical team [1]. Most foreign bodies pass through the gastrointestinal tract without causing any harm, but on rare occasions, perforation can occur. Symptoms are non-specific and can resemble one of many abdominal pathologies [2, 3]. Removal of the foreign body and treatment of the perforation must be performed to avoid potentially fatal complications [4].
CASE REPORT
The patient is a 27-year-old male with no significant past medical history. He presented to the emergency room with a 24-hour history of lower abdominal pain, nausea, and vomiting. On clinical examination, a febrile, tachycardic and dehydrated patient was encountered. He reported pain on his right lower quadrant with a positive Mcburney sign and localized abdominal tenderness. Laboratory blood analyses revealed leukocytosis with neutrophilia. With these findings, acute abdomen due to appendicitis was suspected, and surgery was decided.
Intravenous antibiotics were commenced preoperatively and a Mcburney incision was made, multiple adhesions were found near the cecum, and the cecum wall appeared hyperemic with intense inflammation near the base of the appendix. After blunt dissection, two 3 cm toothpicks were discovered, one that perforated the appendix wall near its base and another one that jeopardized the cecum wall (Figs 1–3).

Two toothpicks, that perforate the appendix and the cecum.

Hyperemic cecum wall with intense inflammation near the base of the appendix.
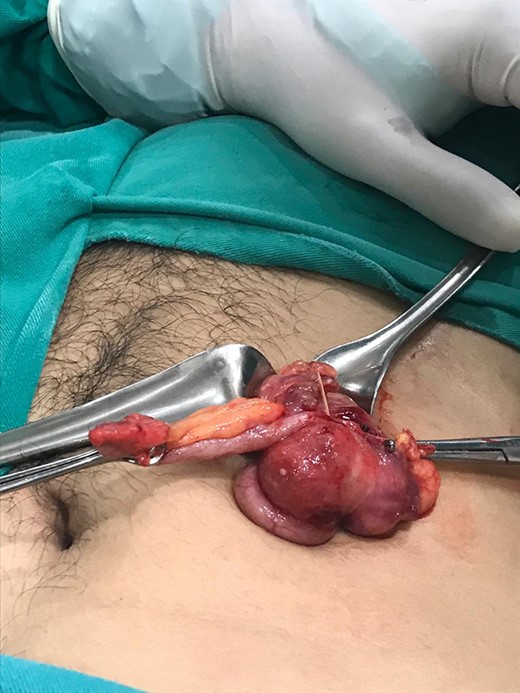
Transoperative image of the cecum and appendix with the two toothpicks.
Surgery was straightforward from this point. The toothpicks were carefully removed, an appendectomy was performed, and the perforation at the base of cecum was repaired with an absorbable suture and covered with an omental patch. An extensive washout with saline solution was carried out and the remainder of the procedure was completed without complications (Fig. 4).

Pathology, appendix wall with acute mucosal inflammation and neutrophilic infiltrates in its wall.
After surgery, the unusual discovery was reported to the patient. However, he didn’t recall swallowing the toothpicks. His postoperative course was uneventful, and he was discharged after a full diet was tolerated. In follow-up controls, the patient shows signs of recovery, and still has no memory of having ever swallowed the toothpicks.
DISCUSSION
Ingestion of foreign bodies is a common event on clinical practice but challenging to diagnose as few patients remember the incident [1]. Risk factors that predispose the ingestion of a foreign body include young age, senility, mental impairments, and alcoholism. However, many ingestions happen on otherwise healthy patients [2], As it happened to our patient. Fortunately, the majority of the ingested foreign bodies are able to transit through the gastrointestinal tract without causing harm [2]; yet, in rare occasions (1%), a life-threatening complication such as a perforation can occur. These perforations tend to happen in regions of acute angulation such as the ileocecum, or in areas near intestinal adhesions, abdominal tumors, hernias, or intestinal resections [2, 3]. It should be noted that the intestine has an exceptional ability to protect itself against perforations. When the mucosa is damaged, an area of ischemia with a central concavity develops at the site of injury, followed by an enlargement of the bowel wall lumen at the point of contact, allowing easier progress of the object [4]. Nonetheless, thin, stiff, sharp, long, pointed, and metallic objects are more likely to cause complications such as intra-abdominal abscess, adhesions, fistulas, and peritonitis [3]. After a foreign body has perforated the bowel wall, it may follow several paths: It may lie in the bowel lumen close to the site of perforation, it may lie free in the peritoneal cavity or migrate into adjacent organs, or it may fall back into the bowel lumen and migrate distally to perforate it again or pass [2]. Symptoms of intra-abdominal perforation by foreign objects are vague and can mimic other causes of abdominal pain, including appendicitis, ureteric colic, inflammatory masses, or fistulas. [2, 5]. Toothpicks, being made of wood, are radiolucent and therefore not usually detected by plain radiographs or computed tomography [6]. Pneumoperitoneum is usually a clear sign of bowel perforation, but since these lesions are caused by impaction and progressive erosion, they allow the omentum or adjacent organs to cover that perforation and limit the passage of intraluminal air into the peritoneal cavity [7]. In our case, due to the clinical findings, acute abdomen was suspected and surgery was decided. As with all other colon perforations, the treatment of cecal perforations should be prompt. The surgical procedure is generally determined by the cause of the perforation; when a small perforation without peritonitis is discovered, a two-layer double-row direct suture can suffice, but in the case of a large perforated section with extensive contamination, the compromised section of the colon must be resected. Depending on the degree of peritonitis, intestinal continuity can be achieved immediately or in a later operation [5]. Open or laparoscopic approaches have been reported for cecal perforations, where the laparoscopic approach has the benefit of shorter hospital stays, less pain, earlier ambulation, better esthetic results and reduced risk of surgical wound infection. Either way, removal of the foreign object and treatment of the cecal perforation must be completed [8, 9]. Toothpick ingestion is difficult to diagnose since most patients do not recall swallowing one, but its occurrence may account for significant morbidity and mortality. Due to its broad spectrum of clinical symptoms, a high index of suspicion is needed and, once suspected, treatment should not be delayed. Surgeons should always keep in mind the possibility of foreign-body ingestion when patients complain of abdominal pain of unknown origin.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}