





Abstract
Situs inversus totalis (SIT) is rare congenital anomaly characterized by an inversion of the thoracic and abdominal viscera that crates a mirror image. Recently, several laparoscopic operations have been reported in patients with SIT. We herein report the case of a 76-year-old woman with ascending colon cancer who received a laparoscopic right colectomy. She was discharged on the 12th day after the operation, without any complications. Laparoscopic surgery in the patients with SIT remains a technical challenge for the surgeon. However, careful understanding of mirror image anatomy and planning of laparoscopic procedure permitted safe operation using technique in ordinary cases. Thus, laparoscopic surgery for colon cancer in the patients with SIT is safe and feasible.
INTRODUCTION
Situs invesus is a rare congenital deformity and is classified as either partial situs inversus or situs inversus totalis (SIT). SIT is characterized by a mirror-image tarasposition of the thoracic and abdominal viscera. Surgical procedures are considered more difficult in patients with SIT in other patients because of different anatomic positions of organs, especially in laparoscopic surgery [1]. Herein we report the case of patient with ascending colon cancer with SIT who underwent a laparoscopic right hemicolectomy.
CASE REPORT
A 76-year-old woman known since early childhood to have situs inversus totalis was referred to the Breast Surgical Department for left breast cancer. She underwent F-fluorodeoxy-glucose positron emission tomography-computed tomography (FDG-PET/CT), because of high level of carcinoembryonic antigen (CEA). PET/CT image showed FDG uptake at the ascending colon (Fig. 1). Therefore, we were consulted by the doctor of Breast Surgical Department. The patient was admitted to our department for further evaluation and surgical treatment. And the treatment for the colon cancer preceded the treatment for breast cancer because of advanced stage of the colon cancer.
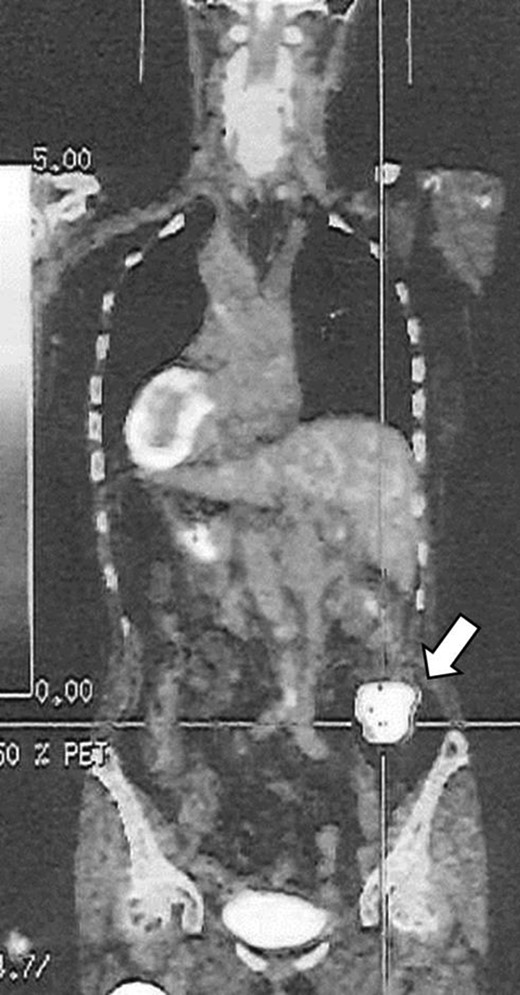
PET/CT image showed FDG uptake at the ascending colon (arrow).
Abdominal CT scan showed complete inversion of the internal organs. 3D-CT angiography revealed no right colic artery and ileocolic artery was located ventral to superior mesenteric vein, and there was angioplany with the exception of mirror image (Fig. 2). Barium enema revealed an elevated lesion in the ascending colon (Fig. 3). Colonoscopy revealed an ulcerative tumor in the adjacent ileocecal valve of the ascending colon; biopsy confirmed that it was a well-differentiated adenocarcinoma. A laparoscopic right colectomy with radical lymphadectomy was performed by ambidextrous surgeon. Under general anesthesia with the patient in a modified lithotomy position, the operator and endoscopist were situated on the right, the first assistant was on the left, the reverse of the locations for orthotopic patients. Trocars also were placed in a mirror image manner, including a 12-mm umbilical trocar for camera, a 11-mm trocar in the right lower quadrant of the abdomen as working port for the operator, 5-mm trocars in the right upper, left upper and left lower quadrant of the abdomen (Fig. 4). The liver was located on the left and the spleen on the right. There was severe adhesion of sigmoid colon and mesentery of terminal ileum to the retroperitoneum. The duodenum had weak fixation to the retroperitoneum and malrotation (Fig. 5). The laparoscopic procedure was commenced breaking up the adhesion of sigmoid colon and mesentery of terminal ileum and retroperitonium. It took almost 40 minutes to break up. We then incised the peritoneal reflection of the terminal ileum to make a tunnel between the mesocolon and retroperitneum until the second portion of the duodenum and head of the pancreas were seen. The ileocolic vessels were identified and divided after the superior mesenteric vein exposed. Dissection of the lymph node started from ileocolic vessels and continued up of the root of surgical trunk (Fig. 6). Next, the remaining ascending colon was fully mobilized along Toldt’s fascia medially to laterally. By extending the 12-mm trocar of the umbilicus, on approximately 40-mm long vertical incision was made, through which we carried the ascending colon include the tumor out. Functional end-to-end anastomosis between the ileum and the transvers colon was extracorporeally performed using staple. No additional port was needed. Operation time was 237 min and the blood loss were 20 ml. Macroscopically, the tumor was a 40 × 40 mm ulcerated lesion in the adjacent ileocecal valve of the ascending colon. Histological examination of the resected specimen disclosed well-differentiated adenocarcinoma. Lymph node metastasis was found in 2 out of 11 nodes (StageIIIB: T3, N1, M0). The patient was discharged on the 12nd day after the operation, without any complication.
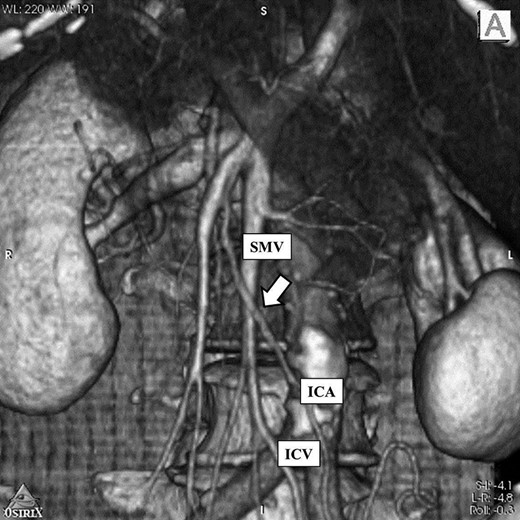
3D-CT image: There was no right colic artery and ileocolic artery was located ventral to superior mesenteric vein (arrow). And there was angioplany. SMV: Superior mesenteric vein ICA: Ileocecal artery ICV: Ileocecal vein.

Barium enema revealed an elevated lesion in the ascending colon (arrow).
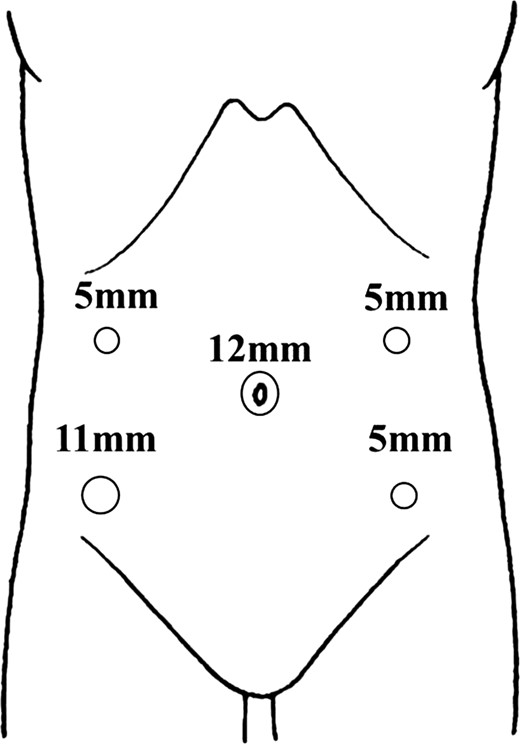
Intraoperative view: trocar placement for laparoscopic right colectomy in this patient.
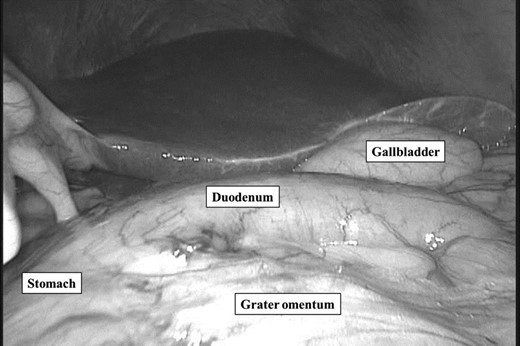
Laparoscopic view: the duodenum had weak fixation to the retroperitoneum and malrotation. The beginning and second portion of the duodenum were abnormal position.
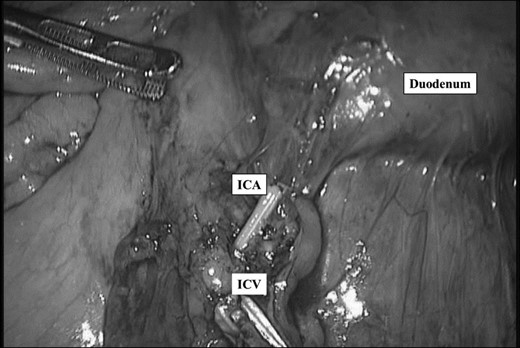
After ligation of ileocecal artery and vein. ICA: Ileocecal artery ICV: Ileocecal vein.
DISCUSSION
The anatomical arrangement of human organs is described by three categories: situs solitus, situs inversus and situs ambiguus. Situs inversus (SI) is a rare congenital deformity. Congenital anomalies, such as syndromes of splenic anomalies and biliary atresia, have been reported to be common in patients with SIT [2]. And intestinal malrotation, an abnormality of intestinal fixation, is characterized by a displaced ligament of Treitz, and also can be accompanied SIT [3]. In our case, the duodenum had weak fixation to the retroperitoneum and there were duodenal malrotation and angioplany. Laparoscopic surgery in patients with SIT remains a technical challenge for the surgeon and is relatively rare [4]. In the colectomy of the patients of SIT, it is anticipated that the surgeon must switch over port for surgeon’s dominant and nondominant hands, which can also cause technical difficulties in patients with SIT, as previously mentioned. Oms and Badia [5] reported that left-handed surgeons have potential advantages in laparoscopic operations for patients with SIT as compared with right-handed surgeons with an unskilled left-handed. However, during laparoscopic operation, surgeons use both hands all the time, so experienced right-hand surgeons also skillfully employ their left hand. Therefore, we consider that right-handedness does not preclude performing laparoscopy. It is important that surgical techniques need to allow for spatial implications of this condition1 and the understanding of the patient’s anatomy, especially vascular structure. Already there are many variations of right side colonic vessels, 3-D CT angiography is useful of understanding of it. Due to careful planning of laparoscopic procedure, and the skillful use of laparoscopy with the left hand, there were no differences in terms of the length of time for surgery, blood loss, and a radical resection of the cancer and accompanying dissection of the lymph nodes, and better results were shown in comparison to previous cases [1, 3]. We agree with this because, after carefully recognizing the mirror-image anatomy, the surgical technique itself did not differ from the typical situation [4]. In our case, although mechanical awakwardness was noted in handling surgical or endoscopic instruments in the presence of reversed spatial relationship, we performed as well as orthotopic cases. Laparoscopic surgery for colon cancer in SIT thus should be considered a feasible safe and curative procedure that surgeons should not hesitate to perform.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}