





Abstract
A 42-year-old lady presented to emergency department with a 3 days history of right-sided abdominal pain. She was afebrile, haemodynamically unstable and the initial diagnosis was acute abdomen with unknown pathology. The CT abdomen/pelvis done, which showed well-defined fatty texture at right lower quadrant suggestive of an epiploic appendagitis and left adnexal cyst. The patient failed to improve on conservative management, diagnostic laparosocopy showed gangrenous sigmoid epiploic appendigitis adherent to the right lower quadrant. Excision of the gangrenous appendigitis done along with deroofing of left ovarian cyst. Postoperatively the patient significantly improved and discharged home. This case is an extremely rare case of right lower quadrant pain. It demonstrates the importance diagnostic laparoscopy in all patients failed to improve on conservative management with presumed appendigitis.
INTRODUCTION
Epiploic appendagitis (EA) are pedunculated adipose tissue that arises from serosa layer covering the colon [1]. There is an estimate of 50–100 appendages extending from cecum to sigmoid [1]. The majority of appendages are located in sigmoid and cecum [2]. The appendages are arranged into two sides of tenia libera and tenia omentalis [2, 3]. Each appendage is supplied by small endarerty from vasa recta of the colon and drained via a single torturous vein through its narrow pedicle [3]. Due to the limited blood supply and shape of appendages, this makes it undergo torsion, which leads to ischemia.
Acute appendagitis is often a neglected differential diagnosis in patients presenting with acute abdomen in emergency department. Moreover, patients usually present with nonspecific clinical signs and symptoms. Patients with EA often present with sudden, focal and severe abdominal pain. The pain is localized usually at right lower quadrant without gastrointestinal symptoms [3].
CASE DESCRIPTION
A 42-year-old Saudi lady with known medical history of hypertension and hypothyroidism presented to emergency department with a complaint of right iliac fossa pain of 3 days duration. The pain was severe in nature, associated with nausea. She denied any history of fever, vomiting, anorexia and changes of bowel habits.
On physical examination, she appeared in pain. She was tachycardiac with 109 beats per minutes and elevated blood pressure of 170/110. Her other vital signs were within normal. Her abdominal examination revealed tenderness and rebound in the right lower quadrant. Chest and cardiovascular examinations were clear.
Upon reviewing her laboratory investigations, C-reactive protein was the only elevated parameter of 18.51 mg/l. All other routine laboratory were within normal range. She underwent a CT abdomen/pelvis, which showed an oval shaped well-defined fatty texture at right lower quadrant measuring 2.8 × 2.4 cm with fat stranding that was suggestive of an epiploic appendagitis (Fig. 1). The CT also noted a large well-defined cyst with a single septum suggestive of left adnexal cyst. A pelvic ultrasound examination showed a cystic structure measuring 6 × 6 cm in left ovary with normal color flow doppler seen.
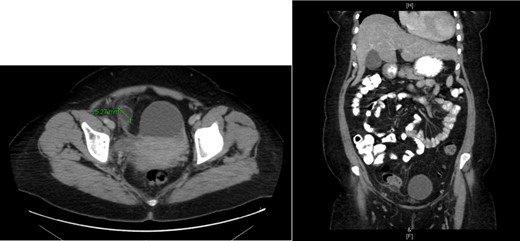
CT showing epiploic appendagitis.
The patient was under the care of Obstetrics/Gynecology and due to persistent pain they elected to take her for emergency laparoscopy exploration. Intraoperative, general surgery team was consulted due to a gangrenous mass adherent to the right lower quadrant abdominal wall, originating from sigmoid colon. The small bowel was inspected from the duodenojejunal junction until the terminal ileum, which was healthy, the colon was inspected until reaching the gangrenous mass, adhesionlysis done and the mass separated from the abdominal wall (Fig. 2). The decision was to proceed for excision of the gangrenous sigmoid appendagitis and deroofing of left ovarian cyst. The postoperative period was uneventful. The histopathology result of specimen reveled necrotic adipose tissue. The ovarian cyst showed a serous cystadenoma.

A laparoscopic view of gangrenous sigmoid appendagitis after adhesiolysis from abdominal wall.
DISCUSSION
Primary EA is an ischemic infraction of epiploic appendages which is a rare cause of acute abdominal pain. Patients usually present in their fifth decade of life with severe pain at the site of infraction [4]. The location of pain was commonly found at left lower quadrant 80% and 14% in the right and only 6% presents with diffuse abdominal pain [5]. Clinical signs and symptoms of EA are nonspecific. Most patients with EA report minimal gastrointestinal symptoms, normal or slightly elevated temperature and leukocytesis [6]. Due to the lack of specific clinical features, EA is rarely diagnosed preoperatively [6].
The clinical presentation of EA can mimic appendicitis and diverticulitis; therefore, radiologist can identify diagnostic CT findings [1]. Contrast enhanced abdominal CT is considered the gold standard when diagnosing EA [7]. Pathognomonic CT findings of EA reveal a pericolonic, oval-shaped, small less than 4 cm, fat density lesions [3, 8]. Nowadays, the increased use of CT as a diagnostic modality aid in the diagnosis of EA preoperatively.
Previously, the standard management of EA was surgical because most cases were discovered during emergency surgery in search of abdominal pathology [8]. Epstein and Lempke were the first to introduce conservative management in 1968 [9]. Some author reported success in nonsurgical management of EA with antibiotics and analgesia [8].
On the other hand, studies have shown that patients may have persisted or recurring pain if managed conservatively, and they supported surgical excision of EA [8, 10].
The case presented highlights the rare presentation of sigmoid EA. Most of the EA mimicking Acute Appendicitis are located in the cecum and most of the EA of the sigmoid are mimicking the diverticulitis presentation. Up to our knowledge from the literature review this is the first case to be reported as Sigmoid EA presenting with acute appendicitis picture.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}