





Abstract
Amyand’s hernia is a rare type of hernia where the appendix is found within the hernial sac. We present a case of appendicitis within an Amyand’s hernia in a 72-year-old man who presented with a acutely painful, irreducible right inguinal lump. He underwent open appendicectomy and primary tissue repair with subsequent delayed elective mesh hernioplasty 3 months later.
INTRODUCTION
Originally described by Cladius Amyand in 1735, Amyand’s hernia where the appendix is found within a hernial sac is a rare finding present in only 1% of inguinal hernias [1]. Finding an inflamed appendix within the hernia is even more uncommon, present in only 0.1% [2].
CASE REPORT
A 72-year-old man presented to a regional Australian hospital with a painful, irreducible right inguinal hernia. He did not have any obstructive symptoms. On examination, he had a 3 cm, tender inguinal lump with overlying skin erythema which was not reducible. He proceeded to CT scan which identified an Amyand’s hernia with radiographic features of appendicitis within the hernial sac with luminal dilation and enhancement of the appendiceal wall (Fig. 1). There was no bowel dilation to suggest obstruction.
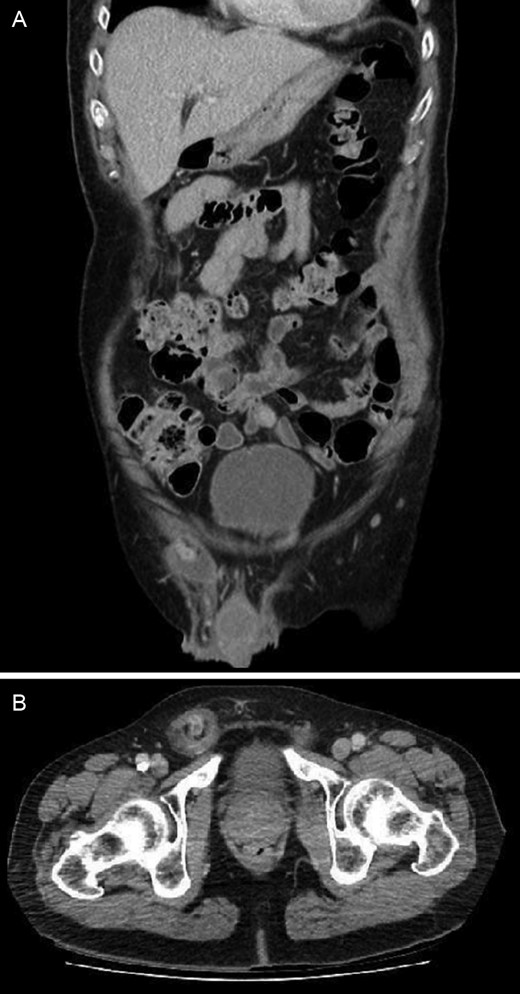
CT showing right inguinal hernia containing contrast filled appendix with dilated lumen, wall enhancement and free fluid within the hernial sac: (A) coronal view and (B) axial view.
He was commenced on intravenous ampicillin, gentamicin and metronidazole and proceeded to the operating theatre. An indirect right inguinal hernia was identified intra-operatively. The hernial sac contained an acutely inflamed appendix and turbid free fluid (Fig. 2). Open appendicectomy and primary herniorrhaphy was performed with excision of the hernial sac and Darn repair. The patient recovered well and was discharged successfully without any complications. Histopathological review of the appendix specimen confirmed acute suppurative appendicitis.
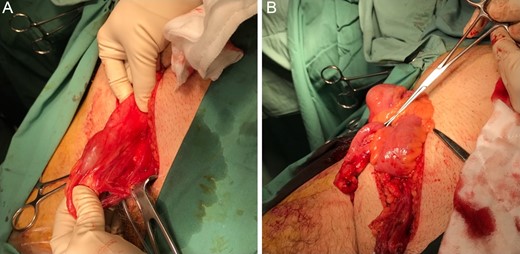
Intraoperative photograph showing acutely inflamed appendix within right inguinal hernial sac (A) and shown after sac opened (B).
The patient returned 3 months later for an elective delayed open mesh hernioplasty with a polypropelene mesh using the Lichtenstein tension-free technique. He recovered well post-operatively without any signs of infection or recurrence on 4 weeks follow up.
DISCUSSION
Appendicitis within an Amyand’s hernia is a rare occurrence and is usually due to incarceration from oedema at the internal ring or contraction of the abdominal muscles at the inguinal canal rather than obstruction by a faecolith [2]. While most Amyand’s hernia are asymptomatic and found incidentally intra-operatively, they may occasionally present with incarceration or strangulation complicated with acute inflammation, abscess, perforation, epididymitis, orchitis or necrotizing fasciitis [3].
The gold standard in managing inguinal hernias in the elective setting is with mesh hernioplasty to minimize the risk of hernia recurrence [4]. This presents a problem when managing Amyand’s hernias where management of the appendix needs to be considered as well. The decision to perform appendicectomy or the presence of appendicitis precludes the use of synthetic mesh due to the risk of mesh infection. Several cases have described the use of synthetic mesh in conjunction with copious wash and antibiotics [5]. The successful use of biological mesh also has been described [2].
Lossannof and Basson described four clinically distinct classifications of Amyand’s hernia with an algorithm to guide management [6, 7]. Type 1 Amyand’s hernias contain a normal, non-inflamed appendix. Reduction of the intact appendix followed by mesh hernioplasty is recommended to minimize the risk of recurrence. Appendicectomy may be considered in younger patients where the risk of developing appendicitis is higher; however, contamination with appendicectomy relatively contraindicates the use of prosthetic mesh. In Type 2 Amyand’s hernias, infection from appendicitis is confined to the hernial sac and patient should undergo emergent appendicectomy through the hernia and endogenous hernia repair. Type 3 Amyand’s hernias have more extensive infection often associated with appendiceal perforation leading to intra-abdominal sepsis or peritonitis and require laparotomy and control of sepsis through debridement, washout or more extensive resection. Endogenous tissue repair of the hernia is usually indicated unless deferment is required in the unstable patient. Type 4 Amyand’s hernias are described where there coexists other complicating intra-abdominal pathology which should be appropriately investigated with a high index of suspicion.
By this classification, our patient had a Type 2 Amyand’s hernia which was managed in the acute setting with appendicectomy and primary tissue repair. He had a delayed mesh hernioplasty to reduce his risk of hernia recurrence as well as risk of mesh infection.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}