





Abstract
The impact of unilateral vocal fold palsy (UVFP) on quality of life cannot be underestimated. Management may be complicated by difficulty in determining prognosis. Currently, there is no standardized management pathway for UVFP. Surgery is considered when speech and language therapy has not been successful or when there is significant aspiration and dysphonia. Surgical options for UVFP include injection laryngoplasty, thyroplasty and laryngeal reinnervation.
We report the case of a 6-year-old girl with a left UVFP sustained following PDA ligation. She suffered significant voice issues, aspiration and intermittent stridor limiting activities. Following multidisciplinary team reassessment including videofluoroscopy and perceptual and objective voice measures, laryngotracheobronchoscopy (LTB) and laryngeal electromyography (LEMG) with injection of Radiesse into the left vocal fold was undertaken. Consequently, she underwent non-selective laryngeal reinnervation with the aim of providing a permanent solution by the formation of an anastomosis between the ansa cervicalis and the main stump of the recurrent laryngeal nerve (RLN) resulting in improved muscle tone.
LEMG indicated no spontaneous recovery. The laryngeal injection allowed for temporary improvement of voice and feeding. Consequently non-selective left laryngeal reinnervation using ansa cervicalis and repeat vocal cord injection was performed. Twelve months following surgery her voice remain greatly improved and there are no feeding issues or aspiration.
In this case so far the use of LEMG and laryngeal reinnervation has proved successful. Non-selective laryngeal reinnervation techniques for UVFP may provide a permanent solution and should be considered in children as a management option in suitable cases.
INTRODUCTION
Unilateral vocal fold paralysis (UVFP) has a significant negative impact on the quality of life for both children and their carers that cannot be underestimated. Children with UVFP suffer from a weak voice affecting their basic communication at home and school, aspiration which requires further interventions such nasogastric (NG) or gastrostomy tube insertion and recurrent chest infections requiring multiple hospital stays. Children with untreated UVFP suffer from social problems, especially when they start school, where the demands on voice are increased [1]. The management of UVFP in children is particularly challenging when compared with adults [2, 3]. Factors that may influence outcome include delays in diagnosis, identification of the functional limitations, the wide range of aetiologies, difficulty in determining prognosis, and the management options dilemmas (Figs 1 and 2).

Approximated left ansa cervicalis branch and left recurrent laryngeal nerve (RLN).
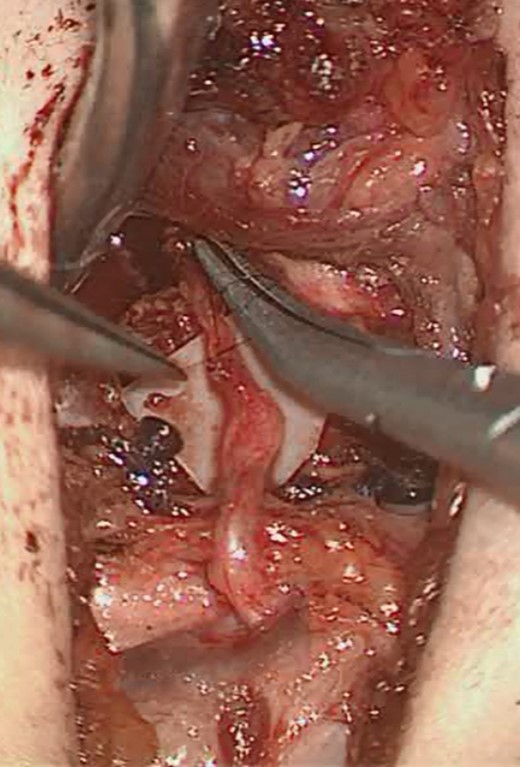
Ansa-left RLN anastomosis.
UVFP in children may be congenital but is more commonly acquired; causes range from birth trauma and iatrogenic (e.g. patent ductus arteriosus ligation (PDA) or repair of a tracheoesophageal fistula) to central pathologies. Indeed studies have shown that the incidence of iatrogenic UVFP following PDA ligation in extreme low birth weight babies (ELBW) (<1 kg) ranges from 22.7–67% [4, 5].
Currently, there is no standardized management protocol for UVFP, as many patients are able to compensate for the glottic defect [6]. Surgery is considered when speech and language therapy has not been successful or when there is significant aspiration and dysphonia [6]. Examples of surgical treatment for UVFP include injection laryngoplasty, thyroplasty and laryngeal reinnervation. Crumley was the first to describe ansa cervicalis to recurrent laryngeal nerve (RLN) neurorrhaphy as a treatment option in children, during the 1980s [7]. The technique of non-selective laryngeal reinnervation involves the formation of an anastomosis between the ansa cervicalis and the main stump of the RLN. This leads to reinnervation of both the abductor and adductor muscle groups therefore improving muscle tone and consequently stabilizing the arytenoid. Non-selective reinnervation is considered a safe procedure based on previous studies and case series [8–13].
We report the first case of unilateral non-selective laryngeal reinnervation in a child in the UK.
CASE REPORT
We report the case of a 6-year-old girl born at 26 weeks gestation. Following PDA ligation at 6 weeks post birth she sustained a left UVFP and required intubation for 5 weeks duration. At 1 year of age, she represented with aspiration, recurrent chest infections, a collapsed right upper-lobe on chest X-ray and required nasogastric (NG) feeding. She was noted to have intermittent stridor limiting activities and a quiet cry. Flexible laryngotracheobronchoscopy (LTB) confirmed a left vocal fold palsy with prolapse of the left arytenoid. Her feeding issues improved after gastrostomy tube insertion. She underwent investigations including videofluroscopy, flexible bronchoscopy, polysomnography and perceptual and objective voice measures. Following removal of the gastrostomy, aspiration became worse. Her voice issues and feeding problems deteriorated affecting both oral feeding with the need for reinsertion of a NG tube and difficulty being heard both in school and at home. At 5 years of age, she underwent rigid laryngotracheobronchoscopy which confirmed no other airway pathology and no crico-arytenoid joint fixation. Laryngeal electromyography (LEMG) and injection of calcium hydroxyapatite (Radiesse) into the left vocal fold was performed during the same procedure. LEMG showed no spontaneous recovery indicating permanent nerve damage and vocal fold injection resulted in an improvement of her voice and resolution of aspiration. Following multidisciplinary discussion with her family, her parents wished to proceed with non-selective left laryngeal reinnervation and repeat injection into the left vocal fold.
A left horizontal neck crease incision at the level of the cricoid was performed. After identification of the internal jugular vein and carotid artery, a branch of the ansa cervicalis was identified, preserved and freed superiorly. The RLN was identified in the tracheoesophageal groove; the left ansa cervicalis branch was divided, trimmed and anastomosed to the divided and trimmed RLN using 10.0 Ethilon sutures and the operating microscope, fibrin glue was used to surround the anastomosis.
Follow up to 12 months postoperatively showed a greatly improved voice that could be heard easily. Paediatric Voice Handicap Index (pVHI) improved from 67 preoperatively to 2 postoperatively and the Paediatric Voice Related Quality of Life (p-VRQOL) improved from 39 to 2. There are no feeding or aspiration problems and her quality of life is greatly improved. Her parents reported ‘Her operation is 100% the best thing we’ve ever done and her voice is 100% better’.
DISCUSSION
In this case, non-selective laryngeal reinnervation has been successful in improving both weakness of voice and aspiration and has had a significant positive impact on quality of life for this child and her family.
There is currently no established preferred surgical intervention for the treatment of UVFP. Reinnervation offers several advantages when compared with its alternatives such as injection laryngoplasty and thyroplasty, especially in children [9]. Injection laryngoplasty has very good outcomes momentarily but results are not permanent requiring repeat procedures under general anaesthesia with the intrinsic risks. Furthermore, the injected material may lead to complications such as inflammation, pain, extrusion of the foreign material and damage to the developing structures. A recent study showed that perceptual and acoustic measurement results from children after reinnervation were better and permanent in comparison with injection laryngoplasty [8]. Thyroplasty is not advocated in children as the laryngeal anatomy alters with growth resulting in failures and further procedures will be needed. Additionally, it is not possible to perform thyroplasty under local anaesthesia in children. Butskiy et al. reported that reinnervation may be the most effective surgical intervention for children with dysphonia, however long-term data are still needed [9].
The decision regarding when to perform non-selective laryngeal reinnervation may be challenging. The procedure has been performed in children at 2 years of age with beneficial outcomes [14]. However, in studies of large groups of children and adolescents with UVFP undergoing reinnervation, there was no correlation between age and postoperative outcomes [10]. Denervation duration did show a slight negative correlation, however improvement was seen in all patients. This suggests that children with UVFP should be offered reinnervation procedures regardless of the length of time since injury with no age limitation for this procedure [10, 13, 15].
CONCLUSION
Our case report has shown that non-selective reinnervation of the left RLN and the use of LEMG has had favourable outcomes for a 6-year-old girl with a UVFP even after a long period of denervation. Non-selective laryngeal reinnervation should be considered as a possible long-term treatment for children with UVFP.
Conflict of Interest statement
None declared.

{kind=link}
{kind=link}