





Abstract
Desmoid-type fibromatosis (DTF) is a rare benign proliferation of myofibroblasts with an unpredictable disease course. Treatment of intra-abdominal located DTF is difficult because of the close relationship with vital organs.
A healthy young male presents with an asymptomatic palpable mass in the lower right abdominal quadrant. A computed tomography shows a 10 × 7 cm2 pear-shaped mass, and pathological examination revealed DTF. A watchful waiting approach was initiated, as the patient was asymptomatic and surgery would imply a significant amount of intestinal resection. After a follow-up of 2 years, the tumor has regressed spontaneously and the patient is still without symptoms.
DTF is a difficult to treat condition where individualized management is appropriate. An asymptomatic patient could be treated with a watchful waiting approach, even with intra-abdominal location. Thereby sparing unnecessary morbidity as the tumor can be stable for many years or even regress spontaneously.
INTRODUCTION
Desmoid-type fibromatosis (DTF) is a benign proliferation of myofibroblasts which can cause significant morbidity by aggressive growth leading to invasion of surrounding organs. Treatment is difficult due to the unpredictable tumor behavior, especially with intra-abdominal location. In this report, we describe a healthy young male with a sporadic intra-abdominal located DTF which was treated with a watchful waiting approach, resulting in a spontaneous regression of the tumor.
CASE REPORT
A 24-year-old healthy male was referred under the suspicion of an inguinal hernia. He was seen at our emergency department with a palpable mass in the lower right abdominal quadrant, which he first noticed 5 days earlier. He had no abdominal pain or symptoms of intestinal obstruction. During physical examination, a non-tender mass was felt which did not increase with the Valsalva maneuver. Sonography revealed a mass of 10.4 × 6.6 cm2. A computed tomography was done for further analysis, and showed an intra-abdominal located pear-shaped mass of 9.5 × 7.1 × 9.1 cm3 along the right ureter and surrounded by small intestines, without invasion of abdominal structures (Figs 1 and 2). It further revealed a congenital malrotation of the small intestine. The differential diagnosis included sarcoma, lymphoma and DTF. A sonography-guided biopsy was performed, and pathological examination confirmed DTF with positive beta-catenin nuclear enhancement. Additional analysis were negative for hormonal receptors. Family history, as well as colonoscopy, were negative for colon polyps. The patient was therefore diagnosed with a sporadic form of DTF. A watchful waiting approach was initiated, as the tumor was asymptomatic and surgery would probably imply significant intestinal resection.
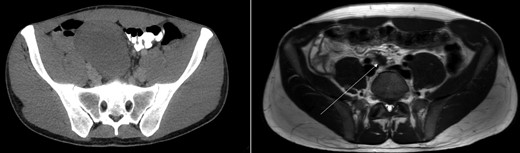
Axial view of CT-abdomen (left) and MRI-abdomen 1 year later. A pear-shaped lesion is seen on the CT, which regressed as seen on the MRI (arrow).
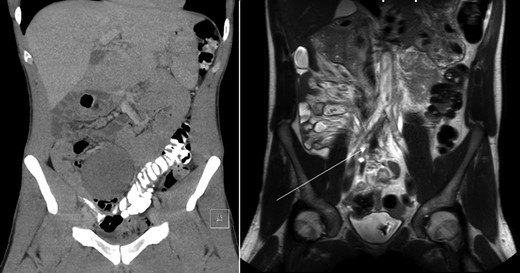
Coronal view of CT-abdomen (left) and MRI-abdomen 1 year later. The lesion has regressed significantly (arrow).
Sonography after three months showed a reduction in size to 9.4 × 5.4 cm2. On request of the patient, who was anxious of having a tumor which was treated conservatively, a second opinion was performed at an University Medical Center. They acknowledged the conservative approach and advised follow up with magnetic resonance imaging (MRI) 1 year after diagnosis. This MRI showed regression of the tumor with a small residue of 2.2 × 1.2 × 1.9 cm2 (Figs 1 and 2) along the right ureter and a minimal hydronephrosis of the right kidney without loss of renal function. A second MRI 6 months later and a third MRI 1 year later showed persisted regression without hydronephrosis. Both scans showed no other masses. The patient did not develop any symptoms during follow up.
DISCUSSION
DTF is a rare condition with an incidence of three per million per year. It can cause significant morbidity and even mortality by local invasion of surrounding organs, but it lacks the ability to metastasize [1, 2].
DTF consists of a proliferation of myofibroblasts and the Wnt/beta-catenin pathway has a central role in tumorigenesis. This pathway is affected by two different mutations. Sporadic cases, the most common form, have a mutation in the beta-catenin gene; cases associated with familial adenomatous polyposis (FAP) have a mutation in the adenomatous polyposis coli (APC) gene [1, 3]. FAP-associated DTF is present in 5–30% of FAP-patients, and is the most common cause of death in this subgroup [1, 4].
The preferred treatment in the past has been surgical, mimicking sarcoma treatment, but contradicting outcomes has changed this approach. Large retrospective series showed high progression-free survival rates in recurrent disease when no treatment was started. These results combined with the higher morbidity after primary surgery due to the spindle-like tumor growth has directed frontline treatment to a watchful waiting approach in asymptomatic patients with sporadic DTF [2]. This change has provided more insight in the natural disease course which includes aggressive growth, but is more frequently stable or with indolent growth. Furthermore, spontaneous regression rates up to 30% have been published, mainly in extra-abdominal or abdominal wall located DTF [5, 6].
Publications of watchful waiting approach in intra-abdominal located sporadic DTF are scarce. The largest study to our knowledge published outcomes of 176 patients (sporadic and FAP-associated) with primary abdominal wall- and intra-abdominal located DTF [7]. An initial observational approach was performed in 109/176 (62%). This was changed to medical or surgical therapy as a result of tumor growth, symptomatic tumor or patient preference in 46% (51/109). A little over a quarter (31/109, 28%) showed stable disease after a median follow-up of 28 months and 23 patients (23/109, 21%) exhibit spontaneous regression after a median follow-up of 49 months. Within the group of spontaneous regression 73% had abdominal wall located DTF. In the end, a total of 67 patients (67/109, 61%) were treated with surgery. This led to a recurrence rate of 24% after a follow-up of 22 months and a second recurrence after surgery in three patients. At last follow-up all the recurrent DTF were stable. Morbidity after surgery has not been described. The article concludes that an initial watchful waiting approach is reasonable to adopt for intra-abdominal located DTF.
The literature provides a variety of treatment options for intra-abdominal DTF [3]. One prospective study from 2012 studied the outcomes of 15 patients with sporadic intra-abdominal located DTF who received surgery as the initial treatment [8]. None were asymptomatic, but only a small group had severe symptoms (pain or melaena). Visceral resection was required in all patients. Complication rate was low with only one bleeding as major complication. After a median follow-up of 40 months, the recurrence rate was 13% which was treated with surgery or medical therapy. There were no deaths. The authors conclude that in intra-abdominal located DTF it is first essential to exclude FAP-associated DTF because this group holds a higher recurrence and complication rate after surgery. With sporadic intra-abdominal located DTF, they advise on a low threshold for surgery.
This case report presents a treatment example conform recently published consensus papers [2]. In here, the authors conclude that asymptomatic patients with sporadic intra-abdominal located DTF should be treated with a watch-and-wait strategy first, keeping them closely followed and adjust therapy to tumor behavior. When tumor growth is seen, surgery remains the standard therapy. In this way, the patient is excluded from unnecessary morbidity after treatment when tumor growth is indolent or even regressive.
CONFLICTS OF INTEREST STATEMENT
The authors have no relationship with a commercial company nor have direct financial interest in the subject matter or materials discussed in this article.

{kind=link}
{kind=link}