





Abstract
Amyand’s hernia is an uncommon form of inguinal hernia. It represents <1% of all hernias and its complication with appendicitis is still rarer with 0.1–0.13% being reported. A 78-year-old woman was taken to the emergency room with pain in the right groin. The patient was assessed by ultrasound with the clinical suspicion of an inguinal hernia. We present the ultrasonographic features of appendicitis within an inguinal hernia sac. A tubular image that terminated in a blind-ended tip in the longitudinal plane and a target image on the cross-sectional plane were consistent with the sonographically demonstrated appendix. The diagnosis of Amyand’s hernia is difficult in the clinical setting. The patient is frequently referred to surgery with the diagnosis of an incarcerated hernia. Ultrasound is a good imaging modality that detects and characterizes this uncommon condition.
INTRODUCTION
Abdominal wall hernias are common findings in surgery; of these, inguinal hernias account for 75%. Inguinal hernias present as a bulge in the groin that disappears when pressure is applied [1]. Approximately 1% of inguinal hernias contain a portion of the vermiform appendix. Amyand’s hernia is an uncommon form of inguinal hernia in which the appendix is incarcerated in the inguinal sac [2]. It represents <1% of all hernias and its complication with appendicitis is still rarer with <0.1 to 0.13% [2]. We present the case of a woman with Amyand’s hernia and appendicitis and the ultrasonographic features of appendicitis in the inguinal hernia sac.
CASE REPORT
A 78-year-old woman was taken to the emergency room because of pain and bulging in the right groin. After evaluation by the emergency physician, the patient was sent for ultrasonographic examination with the clinical suspicion of an inguinal hernia. The patient had a 15-year history of type 2 diabetes, currently treated with insulin, and a 7-year history of hypertension treated with amlodipine 5 mg/day. The patient referred a slow onset with an abdominal stabbing pain of moderate intensity in the right inguinal area and a bulge with no changes in the skin.
Ultrasound findings
Ultrasound was performed with a Philips iU22 ultrasound using a 9 MHz linear transducer. A well-defined cystic mass was observed over the area. Right in the middle, a tubular image that terminated in a blind-ended tip in the longitudinal plane (Fig. 1A) and a target appearance on the cross-sectional plane (Fig. 1B) consistent with the appendix were demonstrated. The appendix measured 0.63 and 0.72 mm, discreetly above normal range, and it showed hypoechoic thickening of the mucosal layer. Color Doppler flow of the tip (Fig. 2) and adjacent soft tissue showed inflammatory changes. The patient presented pain on compression with the transducer. The surrounding fat tissue presented increased echogenicity suggesting inflammatory tissue. The preoperative surgical diagnosis was a strangulated inguinofemoral hernia. However, the findings were reported as acute appendicitis within an inguinal hernia sac. Inguinal hernioplasty with inguinal exploration and repair of an inguinofemoral hernia and resection of intestinal contents were performed (Fig. 3).
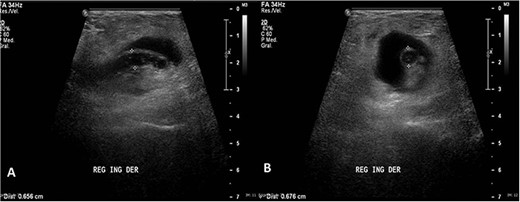
(A) Longitudinal ultrasound of the groin area showing a well-defined cystic mass with a central tubular image that terminated in a blind-ended tip. (B) Cross-sectional ultrasound showing the appendix more than 6 mm in diameter with echogenic surrounding fat soft tissue suggesting inflammatory changes.
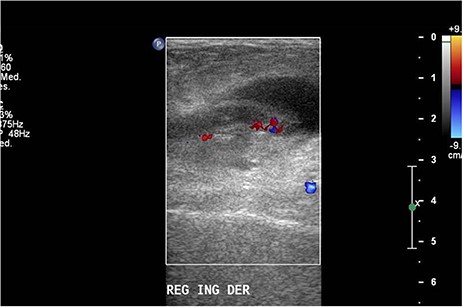
Doppler ultrasound with increased flow on the tip of the appendix.

Cross-sectional incision and dissection of superficial planes; inguinal canal with ordinary content is explored; appendix with gangrenous characteristics within the hernial content. Intestinal resection is performed with appendectomy.
Pathology findings
The surgical specimen received was the cecal appendix with an ovoid shape and measures of 6.5 × 4 × 3 cm. On sectioning, the appendix was 1.2 cm in diameter with a wall thickness of 0.4 cm with a sanguineous secretion inside surrounded by edematous soft tissue and vascular congestion. The section showed the cecal appendix with architectural distortion due to the acute inflammatory infiltrate with neutrophils and eosinophils that destroyed the mucinous secretory epithelium in patches and infiltrated the muscle wall and the adjacent soft tissues forming microabscesses (Figs 4 and 5). The pathology department reported acute appendicitis with microabscesses. The patient was discharged 48 hours after surgery without complications.
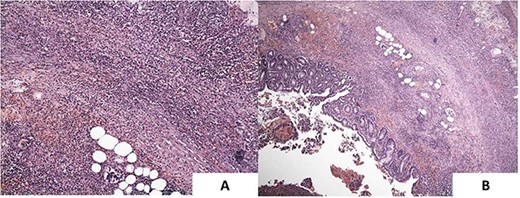
(A) Inflammation extends into the lamina propria. H&E ×100. Large collections of neutrophils are also seen in the lumen and in the muscle layer. (B) The inflammatory infiltrate is predominantly neutrophilic. H&E ×40.
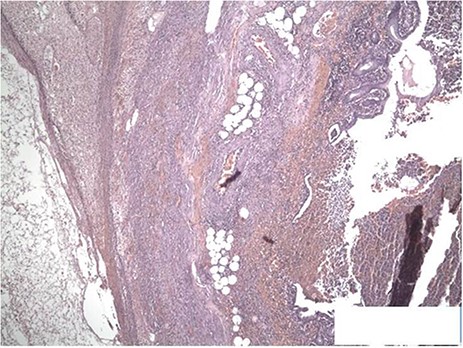
The sections show the appendiceal wall from mucosa to serosa with transmural inflammation. Focal mucosal ulceration is seen as well as congested vessels. Crypt architecture is preserved. H&E ×40.
DISCUSSION
Amyand’s hernia is a rare entity that represents <1% of all hernias. It is more frequently reported in men and on the right side. Complications of this hernia, appendicitis and perforation, are even rarer and have been reported to occur in <0.1 to 0.13% [2]. The reported mortality is 15–30% in most cases as a consequence of abdominal sepsis [3, 4].
After clinical evaluation by the surgeon, the patient was sent to ultrasound with a clinical suspicion of a possible incarcerated inguinal hernia. This common misdiagnosis has been reported in the literature [5]. In general, the clinical diagnosis of this condition is difficult and ultrasound can be a helpful imaging modality to assess the appendix and the hernia sac and to investigate inflammatory soft tissue changes [6]. An important fact to consider in our case is the differential diagnosis with round ligament conditions such as lipomas and varicosities which can also cause severe pain and be confused with appendicitis in women [7, 8]. In this case, the ultrasonographic features allowed us to make the diagnosis of appendicitis within an inguinal hernia sac with high confidence.
We present this rare case of Amyand’s hernia with acute appendicitis to show how ultrasound can be a useful tool in the diagnosis of this disease.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgements
We thank Sergio Lozano-Rodriguez, MD, for his help in translating and editing the manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}