





Abstract
Fibroepithelial polyps (FP) of the ureter are rare and benign mesodermal tumors frequently mistaken for transitional cell carcinoma. We hereby report a rare case of a 19-year-old patient with two FPs, originating from the distal left ureter that were successfully treated with ureteroscopy. One of these polyps was completely protruding outside the bladder through the urethra, which makes this case unique in the literature. Ureteroscopy is currently the best method available for identification, histologic diagnosis and treatment of these polyps.
INTRODUCTION
Fibroepithelial polyps (FP) are benign tumors of mesodermal origin [1]. They are more common in women and are usually located in the proximal third of the ureter (87%) [2]. The left side is slightly more involved and most of the polyps are single, with few cases being bilateral or multiple [1]. Patients usually present with hematuria or flank pain [3]. Excretory urography is the most commonly diagnostic method, solely or in combination with ultrasound, computerized tomography scan or retrograde ureteropyelography (RUPG) [4]. Sometimes the initial diagnosis is very difficult and needless radical surgeries are performed. However, the appropriate treatment remains the endoscopic resection using electro cautery or laser [5, 6].
We are reporting a case of two ureteral FPs with one permanently protruding from the urethra in a young female patient.
CASE REPORT
A 19-year-old female patient, with no medical or surgical history, except tolerated mild left flank pain, presented to our hospital with a mass protruding through the urethra since few days.
She had nor voiding problems neither dysuria. Fever and chills were not reported also.
Physical examination revealed a 2 cm smooth painless red fleshy mass protruding through the urethra most likely originating from the bladder (Fig. 1).
Initial blood tests including chemistry and urinary cytology were normal but urinalysis showed a microscopic hematuria.
Cystourethroscopy revealed a smooth solid pink-colored elongated mass extending from the left ureterovesical junction and occupying the left ureteral lumen.
This mass was easily and completely removed.
Histologically, the tumor had a polypoid structure supported by a large dense hypervascularized fibroconjunctive axis, with normal urothelium and without evidence of malignancy. This finding confirmed the diagnosis of a FP (Fig. 2).

The fleshy red mass protruding from the urethra.
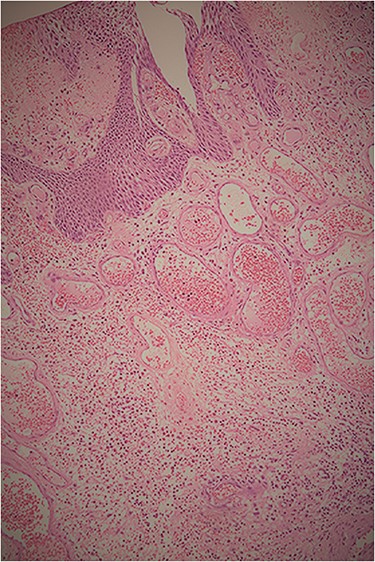
Histopathological examination showing the tumor’s polypoid structure supported by a large dense hypervascularized fibroconjunctive axis, with normal urothelium and without evidence of malignancy.
A post-operative excretory urogram revealed the presence of a distal left ureteral elongated regular non-obstructing filling defect (Fig. 3).
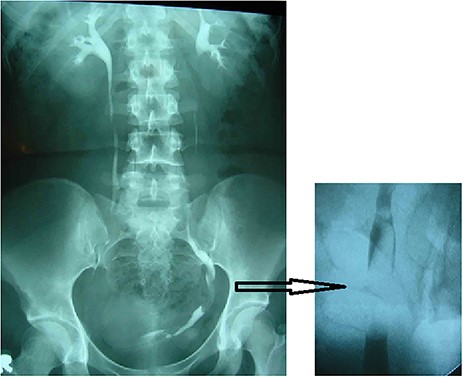
Excretory urogram (left) and RUPG (right) showing the distal left ureteral elongated regular non-obstructing filling defect.
A RUPG, under general anesthesia identified a floating filling defect starting approximately from the mid ureter (Fig. 3).
During the same procedure, a rigid ureteroscope was introduced into the left ureter, 15 cm beyond the ureteral orifice, reaching the origin of the pedunculated mass (Fig. 4A). We did a complete resection of the polyp using electro-cauterization and we inserted a left double J stent.

Endoscopic (A) and macroscopic (B) aspect of the resected FP of the left ureter.
The specimen (Fig. 4B) of solid consistency was macroscopically 6 cm in length with smooth surface and microscopically, similar to the previously described polyp.
The post-operative course was smooth; the double J stent was removed 1 month later without neither any signs of polyp recurrence nor ureteral stricture on the kidney ureter bladder scan done 2 months after the double J removal.
Another computerized tomography urography scan was done 1 year later and showed no recurrence or ureteral stricture.
DISCUSSION
Tumors of the ureter are most commonly malignant and account for <1% of all genitourinary neoplasms. Among the rare non-malignant ureter tumors, FPs are the most common [1].
The exact etiology of benign ureteral polyps is not certain; it is likely that they have a congenital origin. However, chronic irritation and inflammation by agents, such as urinary calculi, was also suggested as a cause for the growth of FPs [2].
Ludwig et al. found 75 articles published during the last three decades and reported 131 cases of ureteral and renal FPs [3]. Flank pain and hematuria were the principle chief complaints of the patients; these symptoms were not present in our reported case. The majority of the cases were diagnosed with intravenous urography, which is also the case of our patient [3].
FPs of the upper urinary tract can cause hydronephrosis in 41.7% of patients [3], which was not the case in our patient. The median polyps’ size was 4 cm, with a maximum reported length of 17 cm [2]; in our case, we had two FPs of 6 cm each.
To our knowledge, there is no previously reported case of a benign ureteral FP with permanent prolapse through the urethra. Our case, although similar in the urographic and endoscopic findings to previous reports, differs from 86.5% of the reported cases in the literature [3] by having two synchronous unilateral ureteral polyps in an asymptomatic patient with a ureteral tumor permanently protruded from the urethra.
These benign tumors are often not easily distinguished from malignant transitional cell carcinomas by clinical or radiologic means; both can present with hematuria, flank pain and filling defect on urography. Urine cytology alone is not a sensitive test and false positive results can lead to unnecessary nephroureterectomy [4]. This is why, it is important to prove the diagnosis of a suspect upper tract lesion prior to adopt the appropriate treatment; specially that histological diagnosis is usually simple and rules out easily the presence of malignant tumors. In our case, the complete protrusion of the polyp from the urethra helped us to have a histological diagnosis before performing ureteroscopy.
So far, there are no guidelines for the management of FPs of the upper urinary tract. Nonetheless, ureteroscopy is still the cornerstone in the diagnosis and treatment of these benign tumors; with recent advances in endo-urologic instrumentation, a diagnostic biopsy and tumor resection are successfully done with no reported recurrences. In our case, we used the cauterization to resect endoscopically the entire polyp, while the Ho-YAG laser was also successfully used by other authors [5, 6].
Recurrence after benign ureteral polypectomy has not been reported and prognosis should be excellent.
CONCLUSION
We report a rare case of a 19-year-old patient with two FPs originating from the distal left ureter. One of these FPs was completely protruding outside the bladder through the urethra. Multiple similar cases of ureteral polyps elongated into the bladder cavity were reported in the literature and only one case report described an intermittent prolapse reaching the urethral meatus; however, our case is the first to report a ureteral FP with permanent extension beyond the bladder cavity through the urethra. Although the diagnosis of these tumors is challenging, ureteroscopy is considered as the best diagnostic and therapeutic tool for their management with minimal risk of morbidity and renal function preservation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}