





Abstract
The role of cytoreductive nephrectomy for metastatic renal cell carcinoma (RCC) is currently debated, with the advancements in target therapy development. The aim of our work was to present an interesting case report with mini review to describe the important role of cytoreductive nephrectomy for kidney cancer control that failed to respond well to Sutent, in spite of good response for all metastases. Medline review of related English publication was conducted and included to the study. RCC response to Sutent is inferior to the response of its metastases. Cytoreductive nephrectomy still plays an important role in metastatic RCC and may be an integral part for cancer control, in properly selected patients.
INTRODUCTION
Renal cell carcinoma (RCC) represents 2–3% of all newly diagnosed cancers, with its incidence and mortality rate being higher in men more than women. Several etiological factors are identified including smoking, obesity, hypertension and family history of RCC in a first-degree relative. Approximately 30% of RCC patients are present with regional or distant metastases, and of patients with localized RCC treated with nephrectomy, 25% are present with relapses in distant sites [1].
RCC has the ability to invade the renal vein and/or inferior vena cava (IVC), and venous tumor invasion has been reported in 10% of patients [2]. Radical nephrectomy with concomitant IVC thrombectomy is then the treatment of choice. This procedure is associated with high mortality and morbidity, with the risk of upward tumor thrombus extension and pulmonary embolism. The availability of molecular-targeted therapies, including Sunitinib, has improved the prognosis of patients with metastatic RCC, with their potential to shrink the tumor and minimize tumor thrombus, which eventually facilitates surgical resection. Moreover, such treatment is appealing because it may allow early treatment of occult micro-metastases improving the curative potential of surgical resection [3].
CASE REPORT
A 58-year-old fit gentleman presented in the mid of 2016 with a large RCC extending into IVC to the liver and multiple lung metastases. It was decided at that time not to do any surgical intervention and to treat solely with Sunitinib. Regular radiological follow-up did show a stable disease, and there was no significant side effects related to Sunitinib. In October 2018, follow-up CT showed complete resolution of lung metastases and extensive thrombus in the IVC extending from iliac bifurcation to the liver, as showed in Fig. 1 [1]. Surgery was done doing radical nephrectomy and complete IVC thrombectomy.
The detailed histopathology revealed a tumor of 10-cm maximum diameter, clear cell, with extensive areas of hemorrhage and necrosis, no evidence of lymphovascular invasion and no rhabdoid or sarcomatoid differentiation, negative surgical margins. The IVC thrombus was all formed of necrotic tissues with no active malignancy. Patient was decided to continue on Sutent after the recovery of surgery. One year follow-up showed no tumor recurrence and normal IVC without thrombus (Fig. 2).
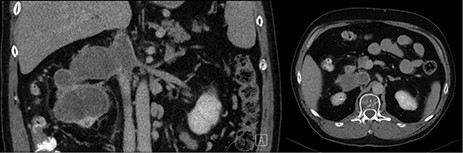
Pre-operative coronal and axial CT images showing right kidney tumor with a large tumor extension into the IVC.
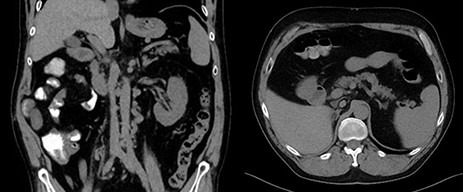
Post-operative coronal and axial CT images showing free tumor bed and normal IVC.
DISCUSSION
IVC tumor thrombus formation in RCC patients is a significant adverse prognostic factor, necessitating an aggressive surgical resection. Many studied have confirmed good outcomes of this extensive surgery for patients with good performance status and absent distant metastases [4]. Sunitinib is an oral tyrosine kinase inhibitor (TKI) that has anti-tumor and anti-angiogenic activity. In patients with metastatic RCC, Sunitinib demonstrated a partial response in 34–40% and stable disease at >3 months in 27–29% of patients [5].
Cost et al. published a retrospective study of 25 patients examining the ability of targeted agents to downsize IVC thrombus. The thrombus level was II in 18 patients, III in five patients and IV in two patients. Sunitinib, Bevacizumab, Temsirolimus and Sorafenib were used in 12, 9, 3 and 1 case, respectively. Thrombus size was reduced in 58% of the patients treated with Sunitinib, but only 31% of those received other agents [6]. Bigot et al. did a retrospective study on 14 patients and found that target therapy has a limited effect on reducing the size of the IVC thrombus [7]. Horn et al. studied five consecutive patients with RCC and level III/IV IVC tumor thrombus, treated pre-surgically with Sunitinib. Four patients showed IVC tumor shrinkage up to 26% cranio-caudally [8]. A case report (2014) of a 62-year-old patient presenting with an advanced RCC, extensive IVC thrombus and lung metastases did show Sunitinib reduced tumor size, IVC thrombus level and the reduced number of lung metastases [9].
A study from Japan described a series of 20 patients who received four cycles of Sunitinib therapy before surgery; in their results, the kidney tumor shrank in four patients, while the IVC thrombus distance above the renal vein was decreased, stable and increased in three, two and two patients, respectively. In this study, one patient had the IVC thrombus mostly replaced with necrotic tissue, while the kidney still had viable tumor cells [3].
Our case is unique that Sunitinib had a very desirable response on lung metastases and converted IVC tumor thrombus into necrotic tissues although it was associated with a cranio-caudal progression in size, followed 2 years of treatment. It was, however, interesting that the kidney still had a viable malignancy, raising the question on the differential effect of TKI on metastases and the primary tumor, and may point to the need to continue doing cytoreductive nephrectomy for these patients with good performance status. Retrospective studies based on large databases suggest longer survival with cytoreductive nephrectomy compared with no surgery (17.1 vs. 7.7 months) with target therapy, in patients with good performance status and low systemic disease burden [10].
CONCLUSION
Sunitinib treatment may help to achieve IVC tumor thrombus necrosis and to cure visible metastases but may not give complete response on the kidney, raising the importance of cytoreductive nephrectomy, in clinically fit patients.
Authorship
All authors helped for manuscript preparation and literature review. Dr Kotb was also responsible for the clinical management of the patient.
Funding
No source of funding.
Conflict of interest
No conflict of interest to declare from all authors.
Informed consent
Informed consent was obtained from the patient.
Ethical approval
Our institution does not require IRB approval for case reports.

{kind=link}
{kind=link}