





Abstract
A thyroglossal duct cyst (TGDC) is a common pediatric midline neck mass. Most TGDCs occur in the region of the hyoid bone but have been found less commonly in areas from the oral cavity to the sternum. We present the first reported case of a multifocal floor of mouth (FOM)/cervical TGDC representing an atypical embryonic course. We also review atypical presentations of TGDC and provide a summary of cases involving FOM and multifocal cysts.
INTRODUCTION
Thyroglossal duct cyst (TGDC) is the most common congenital mass of the neck and occurs due to failure of duct involution after the descent of the thyroid gland from the foramen cecum [1].
Approximately 7% of the population has thyroglossal duct remnants [1]. TGDCs classically present as an asymptomatic midline neck mass that elevates with tongue protrusion or swallowing. These characteristics combined with imaging modalities typically guide diagnosis and treatment of TGDCs. However, while TGDCs are reported to occur in the infrahyoid region in 85% of cases, they have also been described in intralingual, floor of mouth (FOM), suprahyoid, intralaryngeal, intrathyroidal and suprasternal locations [1–6]. Furthermore, this involvement can be multifocal. Awareness of rare TGDC locations is important, as it requires additional investigation to diagnose and treat the thyroglossal duct pathology. We review the less common cyst presentations as well as present the first reported case of a connected, multifocal TGDC that terminated in the FOM.
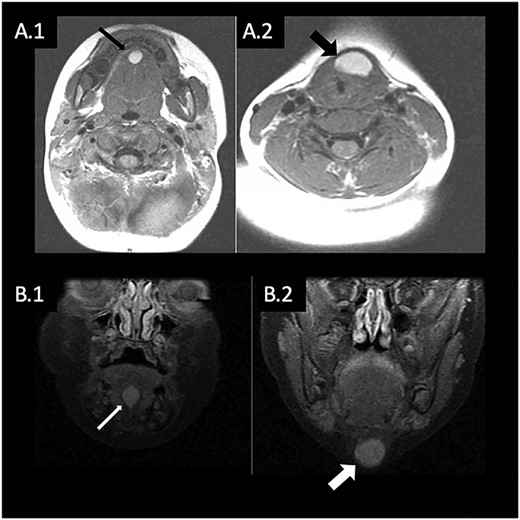
(A) T1 weighted MRI in axial plane showing hyperintense mass in the FOM (A.1) and anterior neck (A.2); (B) T1 weighted MRI in coronal plane showing hyperintense mass in the FOM (B.1) and anterior neck (B.2).
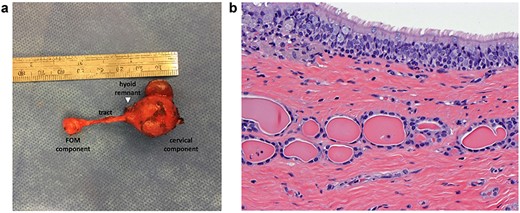
(a) Gross specimen showing multifocal cyst with thin tract. (b) Histology showing cyst lined by ciliated columnar epithelium with thyroid follicles confirming TGDC.
CASE REPORT
A 9-month-old girl presented with a 5-month history of an asymptomatic midline neck mass located at the level of the thyroid gland. The magnetic resonance imaging (MRI) demonstrated a lesion in the anterior neck slightly left of midline, with a second cystic structure incidentally found within the FOM (Fig. 1). The initial differential for these masses included dermoid cyst, epidermoid or rare intestinal foregut cyst. Interestingly, the anterior neck mass showed evidence of a connection to the FOM mass, but no connection to the foramen cecum. As such, TGDC was lower on the differential. An ultrasound again revealed a midline cystic mass extending to the FOM with features suggestive of a dermoid cyst. On repeat physical exam, a small cystic mass in the FOM was palpated, without any obstruction of the oral cavity or airway. Surgical excision of both lesions was recommended. The patient was initially lost to follow up and returned for reassessment at 4 years of age. At that time, there was incremental change in the size of the lesions.
A transcervical approach was utilized and dissection of the midline neck mass revealed a tract extending anterior to the hyoid bone towards the FOM. Because of the close proximity with the hyoid bone, the decision was made to remove the midportion of the hyoid. Once dissection was carried through the mylohyoid, the tract was found to be in continuity with the FOM cyst. There was no evidence of a connection with the base of tongue/foramen cecum. The final specimen revealed a 3.0 × 2.5 × 1.8 cm mass with a 2 cm long tract connecting to the second 1.0 × 1.0 × 0.8 cm mass (Fig. 2a). The specimen was sent to pathology, which revealed a cystic structure with thyroid follicles, confirming the diagnosis of TGDC (Fig. 2b). At most recent follow-up with the patient’s pediatrician 1 year postoperatively, physical exam of the mouth and neck was normal with no evidence of recurrence.
DISCUSSION
During the 4–7th weeks of gestation, the thyroid descends from the foramen cecum and continues inferiorly to the final location within the neck. Involution of the tract occurs during weeks 7–10 of gestation, but failure of involution can lead to the development of a TGDC anywhere along the tract [1]. Although presentation in a pediatric patient is most common, TGDCs sometimes present in adulthood. Management of a TGDC is surgical, with the standard of care being the Sistrunk procedure, which involves excising the cyst, its tract, and the midline portion of the hyoid bone to minimize recurrence [7]. The most common TGDC location reported is infrahyoid, occurring in 65–90% of cases [1–6]. Intralingual TGDCs are rare, occurring in 1–5% of cases [3,4,6]. Intralaryngeal cysts have only been reported in 10 cases and are generally due to enlargement of a TGDC leading to laryngeal invasion [3,4].
Both TGDCs occurring in the FOM and multifocal TGDCs are rare entities. We reviewed six reports of either cysts involving the FOM or multifocal TGDCs. None of these patients had a multifocal cyst that both involved the FOM and required a Sistrunk procedure (Tables 1 and 2). In all of the cases with FOM TGDCs, a transoral incision was used with no reported recurrence [2,4–6]. Two reports stated specifically that no evidence of a tract was seen, which contributed to the decision to forgo a Sistrunk procedure [4,5]. The two additional cases of multifocal TGDCs utilized a transcervical approach with Sistrunk procedure as there was evidence of hyoid bone involvement [7,8]. Our case revealed a multifocal TGDC extending to the FOM with a clear connection between the two masses but with no connection to the base of tongue. This lack of tongue base involvement made the preoperative diagnosis less clear. After a tract with close proximity to the hyoid bone was identified intraoperatively, a Sistrunk was performed to ensure complete excision.
Anterior FOM TGDCs reported in the literature
| Author | Patient age (years) | Sex | Symptoms | Excision approach | Additional findings |
|---|---|---|---|---|---|
| Feunmayor et al. [3] | 45 | Male | Dysphagia, sleep apnea and dysphonia | Transoral | N/A |
| Mukul et al. [5] | 6 | Male | Dyspnea, dysphonia and dysphagia | Transoral | Second recurrence; tract found to extend to base of tongue |
| Nakayama et al. [6] | 6 | Male | Painful swelling and dysphagia | Transoral | N/A |
| 6 | Male | None | Transoral | Concurrent dermoid cyst deep to TGDC |
Radiographic imaging plays an important role in evaluating a neck mass. Imaging can reveal the extent of involvement and aid surgical planning. Ultrasound can be used for typical cases of TGDC and is also useful in confirming the presence of a normal thyroid gland in the case of ectopic thyroid tissue. In the cases of atypical TGDC reviewed here, MRI or computed tomography imaging were obtained to evaluate the masses further. In our case, the FOM mass was only identified after MRI.
Our case represents an atypical course of TGDC. Possible explanations for presentation of a FOM TGDC include ectopic foramen cecum, abnormal descent of the thyroid or branching patterns of the thyroglossal duct [2]. It has been reported that the duct can have multiple branches terminating in blind pouches or connecting with secretory glands [1]. If a transoral incision is made for a FOM cyst, the surgeon should search carefully for an associated tract and complete a Sistrunk procedure if necessary. In our case, the multifocal nature of the TGDC and involvement of the hyoid bone did require a Sistrunk procedure, with the midline portion of the hyoid removed in addition based on our differential of TGDC and the known decrease in recurrence with the procedure.
Conflict of interest statement
None declared.
ACKNOWLEDGMENTS
None.

{kind=link}
{kind=link}