





Abstract
Bezoars, and to lesser extent phytobezoars, are among the rare causes of small bowel obstruction. A bezoar generally describes retained concretions of indigestible foreign material that accumulate and conglomerate in the gastrointestinal tract, most commonly in the stomach. We present an unusual case of phytobezoar-induced sub-acute small bowel obstruction originating from unfamiliar plant material in a 74-year-old woman. The past history was insignificant regarding comorbidities other than depression. Presenting complaints were history of abdominal pain and vomiting. Imaging studies and physical examination suggested small bowel obstruction. The patient underwent exploratory laparotomy after 1 day of conservative treatment. We found a 4.5 cm obstructing phytobezoar intraoperatively. The undigested plant material caused the obstruction. Postoperatively, the plant was identified as Scorzonera papposa. The patient was discharged uneventfully. The elderly patients should avoid semi-cooked vegetables, plants of unknown origin and high-fibre diet.
INTRODUCTION
Bezoar-induced small bowel obstruction is rare and infrequent cause of small bowel obstruction, ranging from 0.4 to 4% worldwide. The bezoars present with similar symptoms as other causes of intestinal obstruction including abdominal pain, vomiting, nausea, dysphagia, loss of weight and inability to pass gas [1]. Hence, bezoars are a challenging cause to distinguish from a preoperative examination [2–4].
There are four major types of bezoars. Phytobezoars comprise undigested vegetable material with large amounts of non-digestible fibres. A variety of fruit and vegetable matter have been found in phytobezoars including persimmons, orange pith, eggplant, grapefruit, mango and carrots [1, 5–7]. Trichobezoars are classically referred to as ‘hair bezoar,’ which are commonly associated with young females and/or patients with psychiatric illnesses such as trichophagia and trichotillomania [2]. Pharmacobezoars are generally caused by conglomeration of medications or medication vehicles such as aluminium hydroxide, antacids and cholestyramine, which in bulk will agglutinate. Finally, lactobezoars affect milk-fed infants [3]. This non-specificity of small bowel obstruction symptoms complicates the diagnosis of bezoars, and its rarity leads to difficulty in tailoring a specific and appropriate management regimen.
THE CASE
A 74-year-orld woman presented to the emergency room with complaints of abdominal pain following a month of recurrent aggravating epigastric distention and repeated vomiting. There was no known history of constipation, loss of weight, diabetes mellitus, hypertension or previous gastric surgery. The patient had been taking psychiatric treatments for depression.
At the time of admission, the patient was vitally stable (temperature 36.9°C, heart rate 82 beats per minute, blood pressure 146/75 mmHg and oxygen saturation 95%). Physical examination revealed mild diffuse abdominal tenderness without guarding or rebound tenderness and hypoactive bowel sounds. The patient was edentulous. The digital rectal examination was normal.
Erect abdominal film demonstrated dilated small bowels alongside the presence of air-fluid filled loops (Fig. 1). Abdominal ultrasound revealed extensively dilated small bowels with multiple gas-filled levels with maximum diameter of 3.5 cm (Fig. 2). Computed tomography (CT) showed the presence of dilated small bowels and local bowel thickening, compatible with the features of small bowel obstruction (Fig. 3). Laboratory data were grossly normal with no evidence of electrolyte abnormalities or increased white blood cell count.
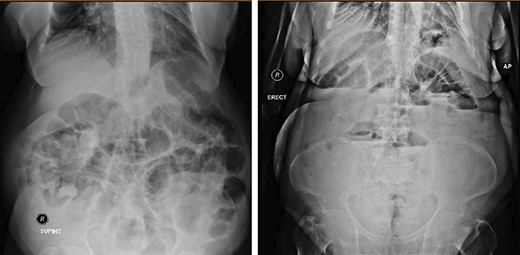
Both supine and erect X-ray show dilatation of the small-bowel.
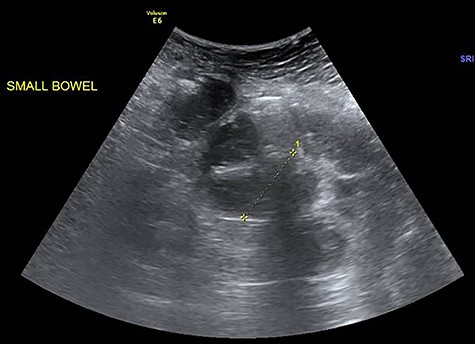
Fluid-filled small bowels with dilatation (widest diameter: 3.5 cm).
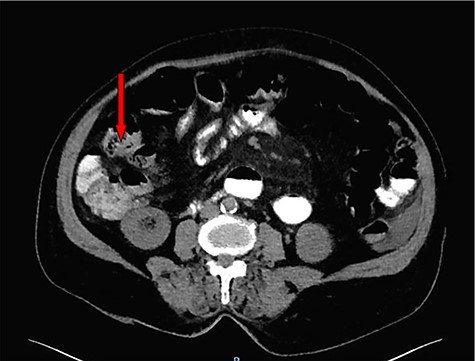
Contrast-enhanced CT scan suggests an appearance of intraluminal debris containing air bubbles ‘mottled appearance’.
Based on the physical examination findings and imaging results, a trial of conservative treatments for sub-acute small bowel obstruction was initiated such as nasogastric tube decompression, intravenous fluids, and repeated gastric lavages. Prophylactic antibiotics were administered for 7 days, but the patient showed no improvement. Consequentially, an exploratory laparotomy was performed. The patient underwent enterotomy revealing a hard 4.5 cm bezoar plug (Fig. 4) obstructing the small bowel (just mention the potion of small intestine usually ileum). The bezoar was composed of indigestible plant materials. Later on, the bezoar was identified as an edible plant known commonly in the Arabian Peninsula as Scorzonera papposa. The procedure was well tolerated, and the patient experienced full recovery postoperatively. During the 3-month follow-up, the patient was well and healed uneventfully.

Retrieved phytobezoar.
DISCUSSION
Intestinal obstruction is a common abdominal surgical disease. According to indexed literature, the aetiologies for intestinal obstruction are varied and diverse. However, it is uncommon for phytobezoar to be a cause of intestinal obstruction. Phytobezoar describes an entrapment of poorly ingested plant fibres, such as fruits and vegetable fibres. The most common cause for phytobezoar was interlinked with ingestion of persimmon fruit [1, 2].
There are numerous predisposing factors that contribute to the formation of phytobezoars. The most common causes are previous gastric surgery, poor dental status, insufficient mastication and metabolic diseases, such as diabetic gastroparesis, chronic kidney disease and hypothyroidism [2]. Diagnosing phytobezoar-induced small bowel obstruction can be challenging preoperatively. Plain abdominal X-ray is nonspecific and gives the picture of minor small intestinal obstruction. On the other hand, abdominal CT has a high sensitivity and high specificity in diagnosing bezoars. However, the gold standard diagnostic procedure for bezoar detection is gastrointestinal endoscopy. In our case, the diagnosis was performed by abdominal pelvic CT scanning [4].
Treatment options for phytobezoar-induced small bowel obstruction are diverse in the literature. Some suggested, especially in case of phytobezoar, that a conservative approach should always be recommended to resuscitate the patient and to prepare a definitive treatment plan. Others preferred a minimal interventional approach through endoscopic fragmentation and extraction, as well as chemical dissolution and repeated lavage. Previous literature shows that surgical intervention via open or laparoscopic techniques is an option for treatment of phytobezoars [5, 7]. However, they are not without disadvantages, such as the need for expertise and the risk of enteric injury due to grossly dilated small bowels [5]. In our case, due to the age of our patient, we successfully dissolved the phytobezoar with repeated gastric lavages.
The definitive treatment option for phytobezoar remains a preventive option. The elderly patients should avoid semi-cooked vegetables, plants of unknown origin and high-fibre diet. Previous literature offers limited approaches to assist those with risk of phytobezoar development, such as ensuring good dietary habits, prophylactic measures to improve gastric motility and psychiatric consultation for those with psychiatric diseases. Our patient was referred to a dietician, as well as consultations in a psychiatric clinic.
To our knowledge from indexed literature, this is the first study to document the presence of phytobezoar in Saudi Arabia. Moreover, this is the first study to describe a phytobezoar originating from S. papposa.
In conclusion, given the rarity of bezoar-related small bowel obstruction and their similar presentation to other small bowel obstruction causes, the diagnosis remains to be challenging and is often delayed. Thus, a clinically unsuspected phytobezoar small bowel obstruction should be considered as a possibility to ensure better management and, consequently, better outcomes.
Conflict of Interest
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}