





Abstract
Congenital anomalies of the inferior vena cava (IVC) are caused by an abnormal persistence or regression of embryonic precursor veins; they are usually incidental findings on imaging studies. These rare conditions have a 0.6% prevalence in individuals with congenital heart diseases and 0.3% in healthy patients. The purpose of this paper was to report two cases of interruption of IVC with hemiazygos continuation and its implications during surgery, highlighting that after recognizing this anomalous drainage the surgeon should be prepared to change the surgical strategies, especially in cardiovascular surgery, in order to obtain adequate circulatory flows or surgical exposure where venous cannulation could be difficult. We have also reported two cases of healthy patients with the same isolated IVC anomaly with no clinical repercussions, which can develop in the future.
INTRODUCTION
The development of the inferior vena cava (IVC) occurs between the 6th and 8th gestational weeks, consists of the growth, regression and fusion of three pairs of embryonic veins (posterior cardinal, subcardinal and supracardinal) [1, 2, 3] (Fig. 1). The anastomoses between the subcardinal veins give origin to the left renal; later, the left subcardinal disappears leaving only the distal portion as the left gonadal; thus, the right subcardinal becomes the main drainage channel and develops into the renal segment of the IVC [1, 2]. The anastomoses of the sacrocardinal veins create the common iliac veins, and when the renal segment is connected to the hepatic segment derived from the right vitelline vein, the IVC is completed, composed of four segments: hepatic, renal, infrarenal and suprarenal [1, 4].
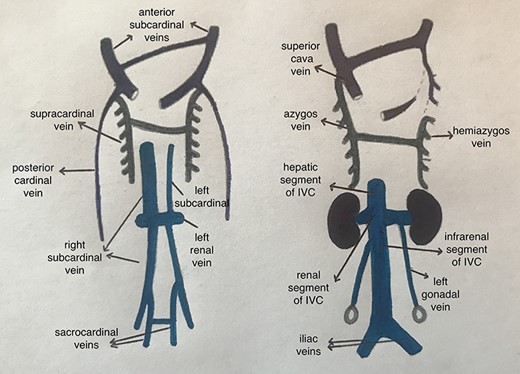
Development of IVC.
CASE REPORTS
Case 1
A 41-year-old male patient with a history of IVC anomaly and interatrial communication, diagnosed when he was 15 years old, was asymptomatic, with no hemodynamic repercussion and good exercise tolerance. Recently presented syncopal episodes and progressive dyspnea due to moderate pulmonary hypertension; despite clinical treatment with sildenafil, symptoms persisted, so he consulted a cardiothoracic surgeon who requested complementary tests. Echocardiogram reported pulmonary artery pressure of 36 mmHg (on Sildenafil) and a left ventricular ejection fraction of 72%. Angiography showed an anomalous distal venous drainage with an absence of the IVC and the persistence of the azygos vein draining distal blood to the superior vena cava (SVC) (Video S1).
With these findings, surgical closure of the atrial septal defect (ASD) was decided; however, due to the IVC anomaly, the surgeon had to modify the surgical technique.
Median sternotomy and systemic heparinization were performed with extracorporeal circulation cannulating the aorta and SVC directing the tip of this cannula to the azygos vein. Right atrium (RA) was opened, the suprahepatic venous system drained into the atrial cavity, complicating the surgical exposure due to the large amounts of blood draining; therefore, these veins were cannulated from the inside of the RA, leaving a bloodless field (Video S2). Chambers were explored, finding a 2-cm ASD and a separate partial anomalous pulmonary venous drainage from the two right pulmonary veins to the RA. The ASD was enlarged with resection of a septal segment; then, correction of the septal communication was performed doing a baffle technique with bovine pericardium creating a tunnel to redirect the flow from the right pulmonary veins to the left atrium (Video S3). Finally, he was removed from extracorporeal circulation and was sent to ICU for postoperative care.
Case 2
This is a 1-month-old male diagnosed with transposition of big vessels, treated with ASA and carvedilol; he was sent to a multispecialty hospital when he was 11 years old. Here, a CT angiogram was donde revealing an ambiguous situs with levocardia, two bilobed lungs, left liver, right stomach, right polysplenia, interruption of the IVC with hemiazygos continuation, four pulmonary veins reached the left atrium, presenting two SVC that reached the RA and IVC interruption with hemiazygos continuation to the left SVC. An ASD was observed, the left atrium communicated with a small and inferiorly situated ventricle, the RA communicated with a larger ventricle of superior situation, with an interventricular communication that can be taken as a single ventricle, transposition of great vessels, the aorta in front of the pulmonary artery. The suprahepatic veins drained directly with a common trunk to the RA. (Video S4).
With these findings, a pulmonary artery–left vena cava anastomosis was performed; his postoperative course was uneventful and was discharged home.
Four years later, the patient consulted because of cyanosis, growth retardation and pulse oximetry of 70%; therefore, a second surgery was decided after right SVC ligation pulse oximetry raised to 90%.
Case 3
A 14-year-old male, without relevant history, consulted the urologist for enuresis and was diagnosed with the right varicocele. CT angiography was performed, showing an IVC anomaly, with partial hypoplasia of the upper segment, persistence of the left SVC to which the left and right renal veins drain, the left renal vein with a retro-aortic segment showing signs of aorto-vertebral impingement, a right dilated and tortuous testicular vein ending in the right renal vein and continuation of the azygos in the visualized thoracic segment. (Fig. 2).
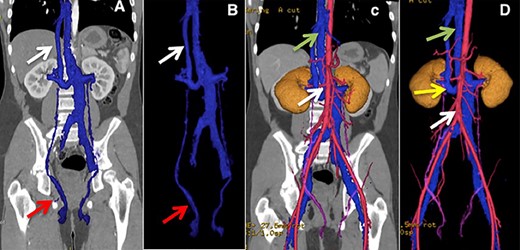
(A and B) Lower arrow shows testicular vein, upper arrow shows hypoplastic suprahepatic segment of the IVC. (C) Lower arrow shows aorta, upper arrow indicates azygos vein. (D) Lower arrow shows aorta, middle arrow shows retro-aortic right renal vein, upper arrow shows azygos vein.
Case 4
A 73-year-old female patient with no relevant history, upper and lower endoscopies were performed due to dyspepsia, biopsies of an anal lesion reported a neuroendocrine carcinoma, in order to stage the malignancy, CT of the abdomen and pelvis revealed a lymphatic mass in front of the sacrum and presence of an anatomical variant of the left IVC, which continues with the azygos vein to the right of the thoracic spine. (Fig. 3).
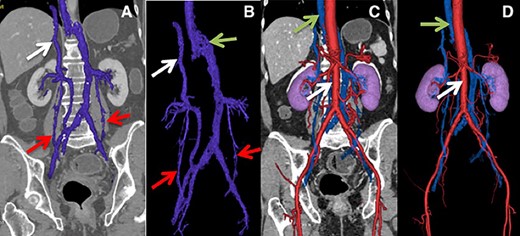
(A) Lower arrows show ovarian veins, upper arrow shows hypoplastic suprahepatic segment of the IVC. (B) Lower arrows show ovarian veins, right upper arrow shows hypoplastic suprahepatic segment of the IVC, left upper arrow shows azygos vein. (C and D) Lower arrow shows aorta, upper arrow shows azygos vein.
DISCUSSION
Interruption of the IVC has an estimated prevalence of 0.6–2% [5, 6] in the presence of cardiac anomalies and less than 0.3% in healthy patients [7]. Most patients with IVC anomalies are asymptomatic when associated with the persistence of azygos/hemiazygos system as in our fourth case; however, in young patients, they could present with acute symptoms of deep vein thrombosis, varicose veins, varicocele [8], as the third patient. The importance of its diagnosis is based on clinical and surgical implications, since they suppose a potential risk of complications in any abdominal/retroperitoneal surgery and especially in cardiovascular surgery [6, 9, 10, 2], such as the first two cases presented in which the surgeon needed to change the surgical technique in order to cannulate the abnormal venous drainage and perform the shunt procedure. Adequate surgical planning based on preoperative CT imaging reconstruction may avoid intraoperative complications or surprises.
Recently, it has been recognized that anomalies of the IVC are an important risk factor for the development of deep vein thrombosis in young patients; despite the prominent collateral veins, they present an inadequate venous return and an increased venous pressure of the lower extremities [4, 8]. Thus, in patients with this type of anomaly, prophylactic antithrombotic measures should be taken in any situation that increases venous stasis [9, 3, 10].
ACKNOWLEDGEMENT
we would like to thank Patricio Velarde, CRNA, for the production of videos for this article and Patricio Silva for the assistance of image reconstructions.

{kind=link}
{kind=link}
{kind=link}