





Abstract
The degeneration of bioprosthetic aortic Conduit with hemodynamic dysfunction mostly requires a re-do surgery, which is associated with an increased perioperative risk. Considering this, an open implantation of a transcatheter aortic bioprothesis (TAVI) after resection of the degenerated valve leaflets could be of great benefit, reducing cross-clamp and cardiopulmonary bypass duration, especially in combined surgery in high-risk patients. This is a case of a high-risk female (78 years, EuroScore 59%) treated with an open TAVI as an alternative to conventional valve or aortic conduit replacement for degenerative aortic valve due to endocarditis lente, 2 years following a bio-Bentall procedure.
INTRODUCTION
Transcatheter aortic bioprothesis (TAVI) procedure is a good alternative to conventional aortic valve replacement in the treatment of aortic valve stenosis in high-risk patients with favorable clinical outcomes. TAVI is applied via several access sites: transfemoral, subclavian, transapical or direct transaortal. The safety of transaortal access has been presented in several studies, and according to literature this approach is associated with a lower rate of perioperative complications.
CASE PRESENTATION
A 78-year-old female, underwent a Bentall procedure for aortic aneurysm and aortic valve stenosis using a bioprosthetic aortic conduit (23 mm Bio Valsalva, Vascutek) 2 years ago, presented with severe aortic and de novo mitral regurgitation caused by a late endocarditis (endocarditis Lente) with Streptococcus sanguinis, diagnosed one year after the initial bio-Bentall procedure and treated conservatively with antibiotics. At admission the patient presented with multiple comorbidities: permanent atrial fibrillation, hypothyroidism, recurrent gastrointestinal bleeding, a previous resection of pancreatic head, cerebral micorangiopathy, lumbar spinal stenosis and polyarthritis.
Over the last 10 months she developed progressive dyspneo with recurrent cardiac decompensation. At admission she presented a functional status of New York Heart Association class III.
Pre-operative trans-esophageal echocardiograms (TEE) revealed severe regurgitation III°–IV° of the aortic bioprothesis and a de novo mitral valve regurgitation III°. The left ventricular function (LVEF) has deteriorated to 40–45% compared to 60% at the time of the initial operation. Coronary angiography showed no evidence of coronary artery disease.
The patient was referred to our unit for urgent replacement of both the aortic conduit and the mitral valve. With regards to the patient’s age, the multiple comorbidities and the perioperative risk (EuroScore 59%) we intended to reduce the cross-clamp and cardiopulmonary bypass duration as short as possible. Previous to the median sternotomy we performed a cannulation of the right axillary artery. The cardiopulmonary bypass was established after cannulation of the superior vena cave and the left femoral vein. The ascending aortic prosthesis was opened with an S-shaped incision, followed by applying of selective cardioplegia (Buckberg).
The inspection of the bioprosthetic aortic valve showed severe degeneration of the valve leaflets by the endocarditis. Vegetations or signs of an active endocarditis were not found (Fig. 1). Taking into consideration the high risk of the combined re-do procedure of aortic conduit replacement and mitral valve repair, we decided to limit our approach to an aortic valve replacement, without the replacement of the aortic conduit in addition to mitral valve repair.
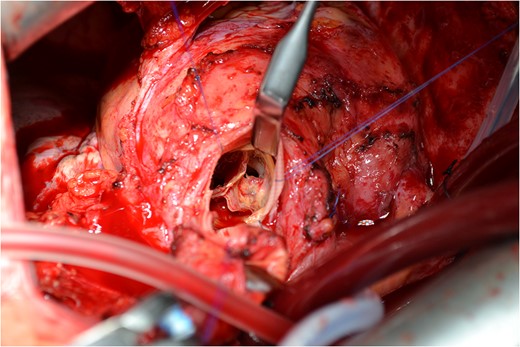
Sever degeneration of the valve leaflets with the formation of perforation in the three prosthetic valve leaflets.
After re-evaluation, we found that an open TAVI instead of the conventional aortic valve replacement would be safer and faster regarding the cross-clamp and cardiopulmonary bypass duration. After total excision of the degenerated aortic valve, a transcatheter bioprosthetic aortic valve (23 mm Edward SAPIEN 3) via a direct aortic approach was implanted (Fig. 2), and the mitral valve was repaired using an annuloplasty ring (EDWARDS PHYSIO II Ring 28 mm). Intraoperative TEE showed a normal function of the implanted aortic valve, and minimal but not relevant central mitral valve regurgitation.
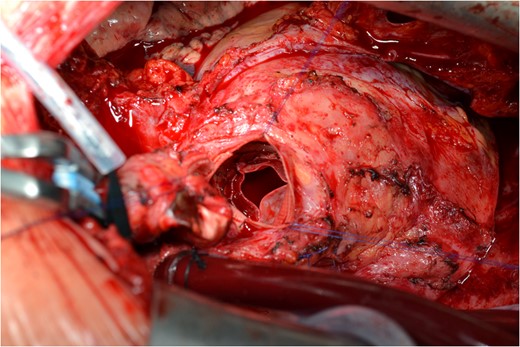
The new implanted aortic valve prosthesis on the aortic conduit.
The patient was extubated on the postoperative Day 1, and remained hemodynamically stable throughout the entire postoperative course. Antibiotic therapy was implemented according to the 2015 Guidelines for the management of infective prosthetic valve endocarditis (PVE) using Flucloxacillin/Ampicillin/Gentamycin. The further postoperative course was uneventful, and the patient was discharged with a slightly improved LVEF after 13 days.
DISCUSSION
Although PVE is a rare complication, it represents a serious issue associated with fatal complications [1]. According to Alonso-Valle et al. [2], the in-hospital mortality was 29%, and 22.91% according to Rekik et al. [3]. In the literature its incidence ranges from 0.1 to 2.3 per patient-year [4]. The TEE represents the standard diagnostic tool for PVE evaluation [5]. The recommended treatment includes first a calculated antibiotic therapy (after the identification of the pathologic germ) and finally the surgical treatment which consists of replacement of the infected tissue and prosthetic material [6].
It is well known that mortality rates are higher in re-do valve surgery than with a primary valve replacement [7]. Furthermore, prolonged cross-clamp time is associated with an increased postoperative morbidity and mortality in both low- and high-risk patients. Our patient may be considered with an EuroSCORE of 59% as a high-risk patient. The operative goal was to repair both aortic and mitral valve failure, and reduce the risk of the re-do operation. The open TAVI of the aortic valve was successful and reduced the cross-clamp and cardiopulmonary bypass duration. The combined procedure of mitral valve repair and open TAVI was performed by an experienced team with no complications. In our opinion this combined minimal invasive approach in the hands of an experienced team represents a reliable method for treating high-risk patients.
CONCLUSION
In summary, we reported a successful re-do operation in a high-risk patient after a late PVE of a biologic conduit with an open TAVI of the aortic valve after the excision of the degenerated bioprosthesis, without the need to replace the previously implanted aortic conduit.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}